Workers' experience of Long Covid
The Covid-19 pandemic continues to impact heavily on all our lives and one of the long-lasting, but unanticipated, impacts is the emergence of Long Covid. Whilst many people infected by Covid-19 may fully recover, significant numbers will experience varied, ongoing and debilitating symptoms that last weeks, months or years following the initial infection. This prolonged condition has been given the umbrella term Long Covid. Recognition of Long Covid was accelerated by people-led advocacy groups such Long Covid Support.3 Their Employment Group (LCSEG)4 advocates for better support to stay in, return to or leave work well.
The Office of National Statistics (ONS) reported that, as of 1 August 2021, 970,000 people in the UK were experiencing self-reported Long Covid.5
The most recent data from 2 January 2023, shows that this has increased to 2 million people6
– this figure is bigger than the population of the cities of Birmingham and Manchester combined. Early research into reinfections 7
shows the risk of Long Covid is still present in subsequent infections, even if not experienced the first time.
This report summarises the findings of a self-selecting survey of 3,097 people with Long Covid in September and October 2022 on their experiences of work.
Treatment at work
Our research found shockingly high levels of poor treatment by employers. One in seven respondents (14 per cent) had lost their job because of reasons connected to Long Covid. Given the high numbers of people experiencing Long Covid, this finding is extremely concerning and many people losing their jobs could be in key sector roles.
Two thirds of respondents (66 per cent) said they had experienced one or more types of unfair treatment at work. This includes one in six (16 per cent) who had been subject to bullying and/or harassment at work, one in 13 (8 per cent) told us they had been threatened with disciplinary action and almost a quarter of respondents (23 per cent) said their employer has questioned whether they have Long Covid and/or the impact of their symptoms.
Half of respondents (49 per cent) said they had reason to believe they had contracted Covid-19 at work highlighting that many people are being continually failed by their employer, from a lack of health and safety measures, including ventilation, to poor treatment in response to Long Covid.
Symptoms
Long Covid is an umbrella term that refers to multiple different symptoms people may experience. Nine in ten (92 per cent) respondents were currently experiencing Long Covid symptoms. The most common symptoms were fatigue (96 per cent), cognitive dysfunction (84 per cent) and shortness of breath or difficulty breathing (73 per cent) amongst a list of many. The range of symptoms experienced by people with Long Covid highlights the need for employers to listen and believe individuals as people’s experiences and the barriers they face in the workplace will be different. Over nine in 10 (93 per cent) respondents also stated that their symptoms fluctuated and over eight in 10 respondents (86 per cent) said they experienced post exertional malaise. This is the worsening of symptoms following physical or mental activity, which can mean that people have to limit their activities and need additional rest periods. Previous research on energy limiting impairments demonstrates that there is much scepticism about the existence and extent of fatigue and a view that it is not a “real disability” creating additional barriers for people who need support from their employers.8
Overall, 60 per cent of respondents said they had been experiencing symptoms for over a year. Six in 10 respondents (63 per cent) told us that their ability to carry out normal day to day activities had been limited substantially and a further third (33 per cent) reported that their ability to carry out day to day activities had been limited to some extent.
Fear of speaking to employers
Our report demonstrated feelings of fear or disillusionment when it comes to speaking to employers about experiences of Long Covid, which is not surprising given the poor treatment revealed. More than one in ten (12 per cent) respondents did not inform their employer of their Long Covid symptoms at all. Of these, a third (36 per cent) said it was because they didn’t think their employer would do anything or they were worried that their symptoms would be viewed negatively by their employer (31 per cent).
Additionally, of the respondents who did share some or all of their symptoms, one third (33 per cent) had not asked for any changes to their job. Of those who had not asked, only one in six (16 per cent) said it was because they did not need any changes. One in three (32 per cent) said they were worried that they would be viewed negatively by their employer.
Accessing changes at work
Of the respondents that did ask, our report reveals the difficulties people are facing accessing the changes and support they need at work and the reluctance of employers to remove barriers to inclusion. Almost half (48 per cent) of respondents reported they were not given all or any of the changes they needed to return to work, and half (50 per cent) were not given all or any of the changes needed to manage their job.
Our findings reveal that employers are seeing standard phased returns to work as the main solution, which, whilst important, fails to recognise the fluctuating nature of the condition. Respondents also reported that flexibility in their role was essential but that this was often the hardest adjustment to get from their employer. Four of the five changes with the biggest discrepancy between being asked for by the person and being put in place by the employer are forms of flexibility: flexibility to support fluctuations in symptoms, longer or more frequent breaks, permanent home working and other changes to hours.
Financial impacts
Our research also exposes the financial impacts of experiencing Long Covid. Half of respondents (50 per cent) said they had to use their savings to financially support themselves, one in sixteen (six per cent) told us they had taken out a private loan or debt service and one in sixteen (six per cent) were using food banks. The report also highlights the difficulties people with Long Covid experience when trying to navigate the social security system.
Our report demonstrates the negative health impacts of poor treatment at work and the process of applying for social security, with respondents reporting relapse and worsening of symptoms.
Context of the research
In June 2021, the TUC and LCSEG conducted a similar survey and produced one of the first reports to demonstrate the impact Long Covid was having on people’s experiences of work. The comparisons between the two surveys reveals how starkly the situation has deteriorated. Half (52 per cent) of the people who responded in 2021 had experienced some form of discrimination or disadvantage, rising to 66 per cent in this survey and 5 per cent had been forced out of their jobs rising to 14 per cent in this survey. The percentage of people not given any or all of the changes they need at work is a notable increase from our 2021 survey (48 per cent of respondents in this survey said they were not given any or all of the changes requested for returning to work and 39 per cent in 2021). These percentage rises are striking and even more concerning as the affected population, as measured by the ONS has also more than doubled.
The impact on work is reflect in national statistics. Over recent years, the number of people in the UK who are out of the labour market has risen sharply. Analysis from the ONS published in December 2022 concluded that Long Covid is likely to be one of the factors contributing to the declining levels of labour market participation during the pandemic.9
However, there has been no targeted government action for people with Long Covid to be able to access and stay in work should they want to.
We have also witnessed some confusion on what legal protections people with Long Covid are entitled to and what employer’s duties are towards them, including whether people with Long Covid are protected under the Equality Act 2010.
People are deemed disabled under the Equality Act 2010 if they have a physical or mental impairment that has a 'substantial' and 'long-term' negative effect on their ability to do normal daily activities.
Whether someone meets the Equality Act 2010 definition of disability 10
would be based on the experiences of that individual. However, our findings indicate that many who responded to our survey would meet it, entitling them to protections and the right to reasonable adjustments. First and foremost, employers should support people in the workplace as it’s the right thing to do, but our results also raise concerns that, by not doing this, many employers could be acting unlawfully.
Both the 2021 and 2023 reports demonstrate clearly that too many people have been and continue to be failed by their employers, in increasing numbers. Many are key workers who kept the country running and yet have been faced with disbelief, negative treatment and a lack of support from employers and government. This report is vital to draw attention to people who have fallen out of work, are underemployed, struggling to remain in or return to work because of the virus.
If we do not take urgent action to ensure that people with Long Covid are properly protected and supported we run the real risk of new, long-lasting inequalities being created with damaging impacts on people’s lives, our economy and our public services, where many of these people are employed.
- 3 https://www.longcovid.org/awareness/what-is-long-covid?fbclid=IwAR0qRlkb88UwkXKOBilwJtUtO8YQCyutlKPBzesEH-6RnGe3nbgTdyQxOhk
- 4 https://www.longcovid.org/about/our-charity#advocacy
- 5 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalnceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/2september2021
- 6 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/2february2023
- 7 https://www.longcovid.org/impact/the-first-ever-data-on-the-effect-of-covid-reinfections-on-people-with-long-covid
- 8 https://chronicillnessinclusion.org.uk/wp-content/uploads/2021/04/energy-impairment-and-disability-inclusion.pdf
- 9 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/selfreportedlongcovidandlaburmarketoutcomesuk2022/selfreportedlongcovidandlabourmarketoutcomesuk2022
- 10 The TUC uses the social model of disability (see the relevant section of the report) meaning we use ‘impairment’ to describe an individual’s physical, sensory, or cognitive differences, and ‘disability’ is caused by barriers in society i.e., being disabled by society. However, the Equality Act 2010 refers to conditions as disabilities. The term disability, rather than impairment, is therefore used in this report when referencing the Equality Act 2010.
Authors
The co-authors of this survey and report from Long Covid Support Employment Group (LCSEG) are Jenny Ceolta-Smith, Polina Sparks, Lesley Macniven, Clare Rayner, and Kirsty Stanley.
As financial and employment impacts on its members became more commonplace, in late 2020 a Long Covid Support Employment group (LCSEG) was formed to meet this need for advocacy. Members of this group, who offer both lived experience and relevant occupational expertise in the areas of HR management, leadership, change management, occupational health, occupational therapy and more, have worked alongside the TUC since March 2021. This is the second survey we have jointly produced, with responses from many of the tens of thousands of people with Long Covid that are supported by Long Covid Support.
As well as the TUC, LCSEG has co-produced resources with the Chartered Institute of Personnel and Development (CIPD), the Society of Occupational Medicine (SOM) and others, all of which are free to download on our website.1
Long Covid Support is a charity registered in England and Wales (1198938) which works across the UK, and internationally, to advance equitable access to high quality healthcare, research engagement, employment rights and welfare services.
The Trades Union Congress (TUC) exists to make the working world a better place for everyone. We bring together more than 5.2 million working people who make up our 48 member unions. We support unions to grow and thrive, and we stand up for everyone who works for a living.
Long Covid Support and the TUC have worked together since March 2021 to highlight the experiences of people with Long Covid and fight for better support for those affected, including to stay in, return to or leave work well.
Acknowledgements
We are grateful to Catherine Hale, former Director, Chronic Illness Inclusion; and members of the TUC Disabled Workers’ Committee who generously shared their insight and expertise with us for this report and to everyone who took the time to complete the survey.
The social model of disability
The TUC and Long Covid Support endorse and use the social model of disability.2 The social model was developed by disabled people to identify and take action against oppression and exclusion. The social model of disability holds that people with impairments are disabled by barriers operating in society that exclude and discriminate against them. For example, barriers can be social and cultural attitudes, organisational and/or physical barriers that prevent equal access. The social model advocates for a “nothing about us without us” approach in which disabled people should have choice and independence, and meaningful input into any decisions being made about them. ‘Impairment’ is used to describe an individual’s physical, sensory, or cognitive differences, and ‘disability’ is caused by the barriers in society.
- 1 www.LongCovidWork.co.uk
- 2 Please see the following documents for further reading on the social model.
Social model of disability: Interactive guide for union reps: https://www.tuc.org.uk/resource/social-model-disability
Trade Unions and Disabled Members: Why the social model matters https://www.tuc.org.uk/sites/default/files/socialmodel.pdf
The Social Model of Disability
Whilst these recommendations are in response to the research on Long Covid, many would also support people with other energy limiting impairments and are informed by best practice in supporting people with other invisible impairments.
Government
Action by government is urgently needed. Without it, we risk people losing their livelihoods as many are forced out of the labour market when they would like to be working and others who cannot work being left with little support.
In all responses, government should ensure that they engage throughout with disabled people, in particular with groups formed by people with Long Covid to represent the community, such as Long Covid Support and trade unions to ensure that the voices and experiences of people with Long Covid are at the heart of all planned activity. Government should:
1. Ensure that everyone with Long Covid is protected under the law by strengthening the Equality Act 2010 by specifying that Long Covid is a disability
This change to the Act could be achieved by using secondary legislation.11
We believe that this should happen for the following reasons:
- We have faced one of the biggest public health crises since the second world war, yet the government has failed to adequately support people facing the long-term consequences of it. Action should be taken to recognise the fact that many people who have Long Covid are key workers who were exposed, and continue to be exposed, to increased levels of risk of Covid-19. Half of respondents in this report said they had reason to believe they contracted Covid-19 at work. Government must ensure that these workers now do not face disabling barriers in workplaces risking their livelihoods.
- Many people with Long Covid will already meet the definition of disability under the Equality Act 2010 and are therefore entitled to additional rights and protections from discrimination. However, many people are not r
- It would ensure that everyone with Long Covid is protected rather than having to evidence that their condition is likely to last 12 months or more. This is particularly important as ONS data from 2022 finds that reporting Long Covid symptoms 30-51 weeks after being infected increases the odds of inactivity by 40 per cent.12
Quick action to ensure people, who want to, can stay in work in their first year after contracting Covid-19 is therefore needed.
2. Provide access to Disablement Benefit
The Industrial Injuries Advisory Council (IIAC)13
has recommended prescription of a number of long-term symptoms associated with Covid-19; designating it an occupational disease for Health and Social Care Workers who have experienced five named complications. An occupational disease is an illness or a condition that can arise or be caused as the result of unsafe working conditions or exposure to certain substances in the workplace and if prescribed, individuals would be eligible for Industrial Injuries Disablement Benefit (IIDB).
We urge the government to accept the recommendation of the IIAC and in addition recognise Covid-19 as an occupational disease beyond health and social care and those five named complications. This would entitle more front-line workers to protection and compensation if they contracted the virus while working and be essential for people who have lost income and work as a result of Long Covid.
3. Protect people from Covid-19 infection
Protecting workers from Covid-19 transmission protects our health, economy and the NHS: it is in all of our interests and is essential to prevent increasing numbers of people experiencing Long Covid. It requires a commitment from the government to invest in necessary resources, and to call on employers to implement protections. The TUC’s A Better Normal report14
outlines the changes we are demanding in relation to health and safety.15
These include removing the ‘lower earnings limit' on statutory sick pay (SSP) and raising the weekly SSP rate to at least the equivalent of a week’s real living wage (£330 per week), which would also mean people with Long Covid would have enough to live on when they need to rest and recover.
One way of bringing the social model of disability into the heart of UK law would be to make the United Nations Convention on the Rights of Disabled Persons (UNCRPD)16
directly enforceable within UK law. Fully incorporating the Convention would bring the added benefit of addressing one of the outstanding recommendations of the UNCRPD to the UK on how to improve and make further progress to meet the Convention’s aims.
5. Strengthen flexible working rights
It is likely that many workers with Long Covid are already covered by the disability provisions of the Equality Act 2010, which would mean that they could ask for changes to their working hours or location as a reasonable adjustment. However, as highlighted in our recent reports on flexible working,17
unless the government acts to strengthen rights and ensure that flexibility is the default way of working, there is a real risk of people not being able to access flexible working due to stigma.
This report shows that while flexibility is one of the changes most requested by people with Long Covid, it is one of the least likely to be approved by employers, potentially forcing people out of the workplace. If the government is serious about supporting disabled people, including people with long-term sickness, it must make flexible working a priority. This would benefit disabled people with other impairments too.
The government must introduce a legal right to flexible work for all workers from their first day in a job18
and a duty to include possible flexible working options in job adverts.19
6. Ensure the welfare system is fit for purpose
There is well documented evidence that welfare reforms in the UK have disproportionately impacted disabled people20
and this report provides further evidence that the system is not working for people with energy limiting impairments. We urge the government to listen the millions of disabled people across the UK, including people with Long Covid,21
and urgently look at how the welfare system can be made better for disabled people. Universal Credit is not fit for purpose - it needs reform in line with recommendations set out in the TUC’s report A Replacement for Universal Credit.22
7. A cross-department approach to Long Covid and continuation of data collection
The response to Long Covid will need to include multiple government departments including Department for Business and Trade, Department for Work and Pensions, Department for Education, Department for Health and Social Care and others and therefore a cross cutting approach to Long Covid is needed. Departments, under the Public Sector Equality, must also demonstrate their due regard for advancing equality of opportunity and eliminating discrimination.
The ONS have also recently announced they are pausing the Covid-19 Infection Survey data collection.23
As demonstrated in this report is has contributed to understanding of the high prevalence of Long Covid and the impact on people’s lives. There needs to be continued monitoring of Covid-19 infections, hospitalisations and deaths alongside ongoing monitoring and reporting of self-reported Long Covid symptoms by the ONS.
8. Invest in regulators
Health and Safety Executive (HSE): The last ten years have seen real-term cuts of 50 per cent to the HSE budget to the HSE budget, 24
with local authorities seeing their inspectorate numbers fall. This must be reversed to ensure safety regulators are well-equipped to investigate workplace health risks and take swift action against employers to prevent poor practice.
Covid-19 has further exposed the need for effective, quality enforcement that rewards best practises and punishes those who put people at risk. This means a long-term investment in the HSE’s inspectorate capacity and local authority environmental health teams to allow for fully trained inspectors, infrastructure and resources needed to keep workers safe.
Equality and Human Rights Commission (EHRC): The EHRC should receive additional ring-fenced resources to use the full range of their powers to address discrimination against people with Long Covid.
9. Strengthen reporting mechanisms
The Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 201325
(referred to as ‘RIDDOR’) plays an important role in collecting data on annual and historical levels of work-related injury and fatalities, triggering investigations into occupational safety, ensuring employers follow protocols, and helping safety regulators direct support and enforcement powers.
Employers are no longer obliged to report cases of Covid-19 infection where exposure occurs as a result of a person's work, unless they are working directly with Covid-19 positive patients, for example in health and social care.
Where a worker is exposed to Covid-19 in the workplace due to lack of effective risk controls, for example, poor ventilation, this should remain RIDDOR-reportable. The TUC’s report ‘RIDDOR, Covid and under-reporting’ argues that Covid ‘clusters’, or outbreaks, in a single workplace should prompt an occupational exposure report.26
10. Provide universal access to occupational health
Only half the UK population has access to occupational health (OH),27
despite its known benefits. OH support could play a pivotal role in supporting people with Long Covid back into the workplace, including atypical workers such as freelancers and agency workers. There should be investment in expert OH advice in government, tax incentives so employers can invest in OH, and access to OH for general practitioners.
Occupational health providers should ensure they are well informed with up to date information and guidance, including information produced with the input of people with Long Covid and bodies, such as the Society of Occupational Medicine28
, who develop guidance with people with lived experience.
The Equality and Human Rights Commission (EHRC
11. Produce guidance for employers
Ahead of legislative change specifying Long Covid as an impairment for the purposes of the Equality Act 2010, the EHRC should urgently work with us to produce guidance for employers. Guidance should focus on reasonable adjustments and best practice, providing detailed examples of different reasonable adjustments people with Long Covid may need in different sectors. Guidance would support employers to take preventative measures to ensure workers with Long Covid do not have to leave the workforce, to protect people’s health and also reduce the risk of potential discrimination by employers. This report highlights the types of reasonable adjustments needed, for example, flexibility, disability leave and a more flexible phased return to work.
We welcome the EHRC’s intervention that states employer best practice is to focus on providing people with Long Covid with reasonable adjustments29
and urge them to build on this. In addition, clarification that a tribunal judgement is not needed for people with Long Covid to receive the protections under the Equality Act 2010 has been useful.30
The guidance should remind employers of their duties under the Equality Act 2010 without the need to go to an employment tribunal.
12. Make targeted use of its enforcement powers
Carry out a programme of targeted work with their full range of enforcement powers to work towards eliminating discrimination against workers who have Long Covid. The EHRC should prioritise strategic litigation on Long Covid, including supporting cases which develop case law around disability discrimination and failure to make reasonable adjustments.
13. Continue to work with Long Covid Support and unions
The ongoing dialogue with the EHRC on Long Covid has been welcomed and we ask that the EHRC continue to work with Long Covid Support and trade unions to implement the above recommendations, including guidance, and promote best practice for employers.
Employers
Employers should focus on providing reasonable adjustments to people with Long Covid and removing barriers for them in the workplace.31
This is essential not only to prevent discrimination and negative treatment at work, but also to ensure that work is not worsening people’s symptoms. This should be done in consultation with trade unions and staff who have Long Covid.
LCSEG have co-created and collated guidance for employers to understand how they can support workers with Long Covid.32
This report builds on that evidence and also contains case studies of the types of support people need. Employers should:
14. Review existing policies, in particular flexible working
Workplace policies should be reviewed in light of this report, in consultation with the relevant unions, workers who have Long Covid and disabled workers. Employers should look at their policies and practices in relation to phased return to work, energy-limiting impairments and redeployment. Our report demonstrates that often people will need longer or multiple phased returns to work due to the fluctuating nature of Long Covid.33
Policies should reflect the fact that some workers might take longer to recover from Long Covid while others might never recover fully or return to their previous ways of working.
Our report shows flexibility is key for workers experiencing Long Covid. Flexibility to organise working hours and workload around symptoms, to rest, to work from home when possible and to have time off to attend hospital appointments is essential to long-term sustainability of work. Employers should review policies to ensure flexible working is the default way of working for all.34
15. Put in place reasonable adjustments for workers who have Long Covid
Our report highlights that in addition to a well-designed phased return to work, adjustments once back at work are vital, yet often employers are failing to provide them. Employers should provide reasonable adjustments to anyone experiencing Long Covid and ensure they are implemented in a timely manner and reasonable adjustment ‘passports’ introduced.35
Employers must recognise that Long Covid is an umbrella term for multiple symptoms therefore no two people with Long Covid are the same and may need different adjustments.
16. Record Long Covid related leave separately from sick leave
Employers should record sick leave taken by workers that is connected to Long Covid separately from sick leave or as disability leave; in line with TUC’s guidance on recording sick leave taken by disabled workers. Education unions have produced a joint protocol on Long Covid which includes this.36
Ensure workers with Long Covid have return-to-work risk assessments
Where it is appropriate for workers with Long Covid to return to workplaces, their condition should be factored into risk assessment and individual risk assessments should be conducted. Research indicates that Covid-19 reinfection can potentially worsen symptoms or cause a recurrence of Long Covid symptoms for people in recovery.37
Certain activities may need to be adjusted on account of symptoms, to avoid risk of injury to the worker or others. For example, some safety-critical functions may not be appropriate for an individual suffering fatigue or cognitive dysfunction.38
Trade unions
Unions should work with employers and people with Long Covid to enact the recommendations outlined above on health and safety, flexible working and other policies to ensure that workers with Long Covid are not discriminated against. Unions should train and develop caseworkers on the strategic use of litigation to tackle all forms of discrimination including Long Covid cases particularly employer failure to provide reasonable adjustments. This will build case law and develop understanding.
Union reps: Unions should use this report and other resources (listed below) to increase their reps’ and members' understanding of Long Covid. There are multiple ways reps can support members to get reasonable adjustments, tackle discrimination, remove barriers in workplaces, and advocate health and safety. Given the fatigue and cognitive dysfunction people may be experiencing, accompanying members to meetings, taking notes, recording decisions and making sure agreements are provided in writing becomes even more important.
This report focuses on recommendations in connection to employment, but we recognise the difficulties that people with Long Covid have accessing healthcare support, as many people with invisible impairments do. Proper resourcing of care and early intervention is needed and can support people to work where this is possible, and they want to return. Long Covid Support39 is involved in such advocacy.
People with Long Covid
If you have Long Covid and need support, the following resources may be of help. If you are a member of a union, contact your workplace rep.
Acas right to reasonable adjustments
CIPD: Working with long COVID: guidance to provide support
Education unions joint protocol on Long Covid
EHRC disability discrimination
Equality Advisory and Support Service
Occupational Therapy for Long Covid PIP guidance
Society of Occupational Medicine Covid-19 return to work guide for managers
Society of Occupational Medicine Long Covid and Return to Work
TUC guidance on improving digital inclusion and remote working
TUC Long Covid: a guide for supporting our members
TUC reasonable adjustments passport
TUC union reps guidance on Universal Credit
TUC webinar on support with Long Covid at work
TUC “You don't look disabled": supporting members with invisible impairments
- 11 https://www.legislation.gov.uk/ukpga/2010/15/schedule/1
- 12 https://twitter.com/JoshMartin_econ/status/1599753864479092737
- 13 https://www.tuc.org.uk/news/ministers-must-not-abandon-workers-long-covid
- 14 https://www.tuc.org.uk/research-analysis/reports/better-normal
- 15 https://www.tuc.org.uk/research-analysis/reports/better-normal?page=4#section_header
- 16 https://www.equalityhumanrights.com/sites/default/files/the-united-nations-convention-on-the-rights-of-persons-with-disabilities-what-does-it-mean-for-you.pdf
- 17 https://www.tuc.org.uk/research-analysis/reports/denied-and-discriminated-against and https://www.tuc.org.uk/research-analysis/reports/disabled-workers-access-flexible-working-reasonable-adjustment
- 18 The current Private Members Bill to make the right to request flexible working a day one night is a step in the right direction but we believe the government must go further. The TUC and Long Covid Support both signed a joined statement calling for this: https://www.fawcettsociety.org.uk/news/response-to-governments-announcement-on-flexible-working
- 19 https://www.tuc.org.uk/research-analysis/reports/disabled-workers-access-flexible-working-reasonable-adjustment
- 20 https://www.inclusionlondon.org.uk/campaigns-and-policy/uncrdp/shadow-report/shadow-report/
- 21 https://committees.parliament.uk/writtenevidence/106644/pdf/
- 22 https://www.tuc.org.uk/research-analysis/reports/replacement-universal-credit
- 23 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19/latestinsights
- 24 https://prospect.org.uk/health-and-safety-executive/
- 25 https://www.legislation.gov.uk/uksi/2013/1471/contents/made
- 26 https://www.tuc.org.uk/research-analysis/reports/riddor-covid-and-under-reporting
- 27 https://www.som.org.uk/universal-access-occupational-health-oh#:~:text=Only%20half%20the%20UK%20population,safely%20during%20these%20challenging%20times.
- 28 https://www.som.org.uk/sites/som.org.uk/files/Long_COVID_and_Return_to_…
- 29 https://www.tuc.org.uk/events/webinar-supporting-workers-long-covid-recording
- 30 https://www.equalityhumanrights.com/en/our-work/news/ehrc-statement-%E2%80%98long-covid%E2%80%99-disability-and-equality-act
- 31 Acas have produced guidance for employers: https://www.acas.org.uk/long-covid
- 32 https://longcovidwork.co.uk/resources/
- 33 This finding concurs with the position paper by SOM https://www.som.org.uk/take-planned-approach-managing-long-covid-workforce-new-som-guide
- 34 TUC’s report The Future of Flexible Working contains more information on how employers can do this. https://www.tuc.org.uk/research-analysis/reports/future-flexible-work
- 35 https://www.tuc.org.uk/reasonable-adjustments-disability-passports
- 36 https://neu.org.uk/management-long-covid
- 37 https://www.longcovid.org/images/Documents/Reinfections_in_Long_Covid_S…
- 38 https://www.som.org.uk/take-planned-approach-managing-long-covid-workforce-new-som-guide
- 39 https://www.longcovid.org/about/our-charity#advocacy
The Covid-19 pandemic continues to impact heavily on all our lives and one of the long-lasting, but unanticipated, impacts is the emergence of Long Covid. Whilst many people infected by Covid-19 may fully recover, significant numbers will experience varied, ongoing and debilitating symptoms that last weeks, months or years following the initial infection. This prolonged condition has been given the umbrella term Long Covid or sometimes referred to as post-Covid-19 syndrome or post-acute sequelae of Covid-19. The National Health Service (NHS) advises contacting a general practitioner (GP) if someone is worried about symptoms four weeks or more after a confirmed or suspected Covid-19 infection. 40 The National Institute for Health and Care Excellence guidelines includes acute Covid-19 (up to four weeks), ongoing symptomatic Covid-19 (symptoms from four to 12 weeks) and post-Covid-19 syndrome (symptoms past 12 weeks).41
Throughout this report we refer to Long Covid as this is the term created by people experiencing the symptoms.
Long Covid is an energy limiting condition and an umbrella terms that refers to multiple different symptoms; a study led by a patient led research collaborative identified more than 200 possible symptoms.42
However, some of the more common symptoms are energy exhaustion (fatigue) 43
, shortness of breath or difficulty breathing, cognitive dysfunction and muscle pain and aches44
and symptoms are likely to fluctuate.
There is evidence that demonstrates the number of people impacted by Long Covid is increasing. The ONS reported that as of 1 August 202145
970,000 people living in private households in the UK (1.5 per cent of the population) were experiencing self-reported Long Covid. The most recent data from 2 January 2023 highlighted that this had increased to 2 million people (3 per cent of the population).46
Anyone can be affected by Long Covid but there is a higher prevalence of self-reported Long Covid in certain groups. The latest ONS data shows that they are people aged 35–69 years old, women, people living in deprived areas, those working in social care, people aged 16 years or over who were not working and not looking for work and disabled people.47
Previous data sets have also included people in health and education.
However, an ongoing issue when analysing the disproportionate impact of Covid-19, is a lack of public understanding on what constitutes Long Covid, the difficulty in gaining a diagnosis, the range of symptoms people can experience and that some people would not have had a positive Covid-19 test due to the difficulties that many experienced in accessing tests at the start of the pandemic and the ending of free testing in 2022. This is likely to impact people's ability to report it accurately.
Over the last three years, we have seen the huge impact that Long Covid is having on people, including their experiences of work. The TUC and Long Covid Support published results from a survey June 202148
and this report is an effort to build on that evidence with the aim of ensuring that people are properly supported in the workplace.
This report is broken up into the following sections:
- Section 1: Background - relevant legislation and experiences of disabled people
- Section 2: What we know so far - Covid-19 and Long Covid and work
- Section 3: Methodology
- Section 4: Findings - Long Covid symptoms
- Section 5: Findings - Experiences of work
- Section 6: Findings - Financial support
- Section 7: Findings - Experiences of unemployed people
- 40 https://www.nhs.uk/conditions/coronavirus-covid-19/long-term-effects-of-coronavirus-long-covid/#:~:text=What%20is%20long%20COVID%3F,or%20post%20COVID%2D19%20syndrome
- 41 https://www.nice.org.uk/guidance/ng188
- 42 https://patientresearchcovid19.com/publication/
- 43 Fatigue described by people with Long Covid is often met with scepticism and a response of ‘we’re all tired’. One of the authors of this report described her fatigue as like operating a device on a faulty battery - at some point non-essential functions fail for it to just keep running and ultimately it shuts down and everything powers down. It then takes forever for the battery to re-charge, doesn't hold the charge, and quickly discharges again. “I feel like I’m on battery saver mode and certain functions just don’t work and can’t recover.” ‘The Spoon Theory’, coined by Christine Miserandino in 2003 is another analogy also used by disabled people to describe energy limiting fatigue.
- 44 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1december2022
- 45 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/2september2021
- 46 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/2february2023
- 47 Ibid
- 48 https://www.tuc.org.uk/research-analysis/reports/workers-experiences-long-covid
Disability provisions in the Equality Act.
Disabled people are protected by the Equality Act 201049 from discrimination in employment and a range of other areas including education, provision of services and transport. All employers have a legal duty under the Equality Act 2010 to proactively make reasonable adjustments to remove, reduce or prevent any disadvantages that disabled workers face. The Equality Act 2010 protects people from discrimination so it is not applicable only to employees as some employment law is.
The Equality Act defines disability as a “physical or mental impairment…[that] has a substantial and long-term adverse effect on [their] ability to carry out normal day-to-day activities”.50 Government guidance makes clear that 'substantial' means more than minor or trivial and if you are having treatment for the condition this is discounted; the impact is without treatment or medication.
'Long-term' means the effect of an impairment has lasted for at least 12 months, is likely to last for at least 12 months or is likely to last for the rest of the life of the person affected. In addition, likely means ‘could well happen’51 and day to day activities are things people do on a regular or daily basis with examples given such as shopping, reading or writing.
The guidance also highlights the importance of considering the cumulative impact of multiple impairments that a person might have and states that even if individual impairments might not have a substantial impact if considered in isolation “account should be taken of whether the impairments together have a substantial effect overall on the person’s ability to carry out normal day-to-day activities”.52 In addition, there is specific guidance on recurring or fluctuating conditions stating that if the impacts of an impairment cease but are likely to reoccur, they will be treated as continuing to have that effect.
Some disabilities, for example HIV, cancer and multiple sclerosis are named disabilities and are automatically covered by the Equality Act 2010 meaning workers benefit from the disability provisions within the Act from the point of diagnosis.53
Whether someone with Long Covid is deemed disabled under the Act and therefore entitled to the protections, will therefore, as with any other impairment (other than those named in the Act), be dependent on whether they meet the definition outlined. As Long Covid is a new condition there has been confusion about this, so it is important to remember that employers have the same duties under the law as they do to other disabled people.
Under the Act there are six main types of discrimination that disabled people are protected from. They are direct discrimination, indirect discrimination, failure to make reasonable adjustments, discrimination rising from a disability, harassment and victimisation.54
The EHRC has recommended that to support someone with Long Covid and avoid inadvertent discrimination, employers should follow the existing guidance on reasonable adjustments and access to flexible working55 and best practice is to focus on providing reasonable adjustments and support to the person experiencing symptoms.56
It is important to note that a medical diagnosis of Long Covid is not needed to meet the definition as the focus is on the impact of the impairment. 57
There has been debate on whether someone with Long Covid needs to take a case to an employment tribunal to demonstrate if they are entitled to disability protections under the Equality Act 2010.58 We welcome clarification from the EHRC that a tribunal judgment is not needed for an employer to provide support and Long Covid will count as a disability for a particular person if their condition meets the Equality Act definition.59 Confusion over this is important to clarify as it could result in employers believing that a tribunal case is required before they make any adjustments for workers with Long Covid – this would be a unique and unjustified exception to the Equality Act 2010 and is not correct.
T
If a case were to end up at a tribunal, it is the definition under the Act that would be used in making a judgement on whether disability discrimination has occurred. There have now been employment tribunal judgements where the claimant with Long Covid was deemed to be disabled.60
The duty to make reasonable adjustments.
The Equality Act 2010 recognises that to bring about equality for disabled people, changes or adjustments to workplaces or working arrangements may be needed. This is the duty to make reasonable adjustments.61 The duty means that disabled people can be treated more favourably in order to reduce workplace disadvantage.
Reasonable adjustments are changes to work environment or to a workplace policy, process, criteria or practice that removes or reduces disadvantage that disabled people face at work. They could include for example changes to someone’s working arrangements like their hours or location, providing equipment, making physical changes or findings a different way to do this. This report outlines the reasonable adjustments that people with Long Covid may need, but everyone's’ adjustments are individual, and can cover any area of work.
Employers have a duty to provide reasonable adjustments when they know or could reasonably be expected to know someone is disabled. They must provide them to employees, workers, contractors, self-employed people, trainees, apprentices and job applicants. Reasonable adjustments are a day one right and what is reasonable depends on each situation. But if an employer fails to make a reasonable adjustment, a person could make a disability discrimination claim to an employment tribunal.
Social model of disability
This report has outlined the legal protections that people with Long Covid are entitled to. Another way to support people is the use of the social model of disability, which the TUC and Long Covid Support endorse 62 . The social model is endorsed by the UNCRDP and is an alternative to the medical model of disability, on which the Equality Act 2010 is based.
The social model of disability was developed by disabled people to identify and take action against oppression and exclusion. The social model of disability holds that people with impairments are disabled by barriers operating in society that exclude and discriminate against them. For example, barriers can be social and cultural attitudes, organisational and/or physical barriers that prevent equal access. The social model advocates for a “nothing about us without us” approach in which disabled people should have choice and independence, and meaningful input into any decisions being made about them. ‘Impairment’ is used to describe an individual’s physical, sensory, or cognitive differences, and ‘disability’ is caused by the barriers in society.
The government and employers adopting the social model 63 is vital to support people with Long Covid symptoms as it focuses on removing barriers that people experience which prevent them from working well. The government should also move away from the medical approach to disability as set out in the Equality Act 2010 and adopt the social model of disability as outlined in the recommendations of this report by implementing and directly incorporating the UNCRPD into domestic legislation.
Treatment of disabled people with energy-limiting impairments
In seeking solutions to the negative experiences of people with Long Covid at work, it is vital to ground all solutions in the lived experiences and preferences of people who have Long Covid. However, it is also important to reflect on the previous experiences of disabled workers with energy limiting impairments, such as severe fatigue. It is estimated that around 250,000 people in the UK experience myalgic encephalomyelitis (ME) or chronic fatigue syndrome (CFS).64
ME or CFS is a long-term, fluctuating, neurological condition that causes symptoms affecting the nervous and immune systems. People with ME/CFS experience debilitating pain, fatigue and a range of other symptoms associated with post-exertional malaise. This is the body and brain’s inability to recover after expending even small amounts of energy. Not everyone will experience the same symptoms. Reports and data about Long Covid symptoms and patient experiences contain many similarities to other chronic illnesses known to be associated with viral triggers, such as ME/CFS.
Workers with energy impairments have faced widespread discrimination and disbelief at work. Scepticism about the existence and extent of energy impairments like ME/CFS is widespread as highlighted in a report by Chronic Illness Inclusion65 which stated that “negative perceptions and misunderstandings around ‘fatigue’ and chronic illness create formidable yet unnecessary barriers to work. The widespread notion that fatigue is not a real disability stands firmly in the way of disability equality in work. Systemic disbelief of energy impairment affects disability disclosure and access to reasonable adjustments, and contributes to strained employment relations, sometimes causing unnecessary departure from the labour market.”
The parallels between workers with other energy limiting impairments and Long Covid are clear. Going forward it is imperative employers understand energy impairments and learn the lessons from experiences of people with ME/CFS and Long Covid and vice versa, so that appropriate reasonable adjustments are put in place for workers.
Social security
Our survey includes questions on what financial support respondents were accessing, including whether they were accessing support from the Department for Work and Pensions (DWP). Having a diagnosis of Long Covid does not necessarily lead to social security entitlement. There are different financial entitlements (income-related and contribution-based) that working age people in the UK may be eligible to apply for. Eligibility criteria is specific to each benefit and can include, for example, the nature of a person’s impairment and, or health condition, partner status and living arrangements, having dependent children, financial circumstances, and current and recent past work situation
People with Long Covid have reported challenges in applying for DWP support, particularly about the required medical assessments. Long Covid Support
A key social security entitlement that is likely to be applied for by people with Long Covid is personal independence payment (PIP) in England and Wales and recently changed to adult disability payment (ADP) in Scotland.
Other key entitlements that people with Long Covid may be claiming include
A section on industrial injuries disablement benefit is included later in this report.
- 49 https://www.legislation.gov.uk/ukpga/2010/15/section/6/enacted
- 50 Ibid
- 51 https://www.gov.uk/government/publications/equality-act-guidance/disabi…;
- 52 Ibid
- 53 These are covered in Schedule 1, Part 1 of the Equality Act 2010 and in Regulation 7 of the Equality Act 2010 (Disability) Regulations 2010.
- 54 https://www.equalityhumanrights.com/en/advice-and-guidance/disability-discrimination#:~:text=The%20Equality%20Act%202010%20says,known%20as%20discrimination%20by%20association)
- 55 https://www.equalityhumanrights.com/en/our-work/news/ehrc-statement-%E2%80%98long-covid%E2%80%99-disability-and-equality-act
- 56 https://www.youtube.com/watch?v=nBObcrblbrU
- 57 Ibid
- 58 https://www.theguardian.com/society/2022/may/09/alarm-after-ehrc-says-long-covid-should-not-be-treated-as-disability
- 59 https://www.equalityhumanrights.com/en/our-work/news/ehrc-statement-%E2%80%98long-covid%E2%80%99-disability-and-equality-act
- 60 https://www.gov.uk/employment-tribunal-decisions/mrs-h-matthews-v-razors-edge-group-ltd-2409756-slash-2020 and https://www.gov.uk/employment-tribunal-decisions/mr-t-burke-v-turning-point-scotland-4112457-slash-2021
- 61 https://www.acas.org.uk/reasonable-adjustments
- 62
Please see the following documents for further reading on the social model.
Social model of disability: Interactive guide for union reps: https://www.tuc.org.uk/resource/social-model-disability
Trade Unions and Disabled Members: Why the social model matters https://www.tuc.org.uk/sites/default/files/socialmodel.pdf
The Social Model of Disability
- 63 https://www.tuc.org.uk/resource/social-model-disability
- 64 https://www.nature.com/articles/s41579-022-00846-2
- 65 https://chronicillnessinclusion.org.uk/wp-content/uploads/2021/04/energ…
- 66 Written evidence on Health assessments for Benefits for the Works and Pensions Committee https://committees.parliament.uk/writtenevidence/106644/pdf/
- 67 https://www.gov.uk/universal-credit
The impact of Long Covid on employment and the economy
With prevalence of Long Covid being highest in 35-69 year olds and in social care, health and education sectors, the potential impact on the economy is significant.
Our 2021 report on workers’ experiences of Long Covid found that one in 20 (5 per cent) respondents had been forced out of their jobs because they had Long Covid and over half of respondents (52 per cent) said they had experienced one or more of the types of unfair treatment at work, including one in six who were concerned that having Long Covid had affected their chance of a promotion and one in 25 who said they had been forced to take additional unpaid leave as a result of having Long Covid. This indicates the impact that Long Covid is having on people’s ability to progress, work enough hours and stay in work altogether.
We are also seeing these trends worldwide; an international study reported that 42.5 per cent of people with Long Covid had to reduce their work schedule compared to the period before having symptoms and 22.3 per cent were not working due to various reasons such as sick leave, dismissal or resignation.68
In total, there are 440,000 more people who are economically inactive in the UK now than before the Covid-19 pandemic began; that is, they are neither in work nor looking for work. This increase was primarily the result of an increase in the number of people who are out of work because of long-term ill health.
The number of people who are out of work and not looking for work because of poor health, although just below the peak reached in the third quarter of 2022 remains significantly higher than it was going into the pandemic, rising from 2.1 million in the first quarter of 2020 to 2.5 million in the fourth quarter of 2022 (as shown in Graph I).69 This has been linked to older workers’ ill-health,70 NHS waiting lists, a rise in mental distress and Long Covid.71
Figure I: Number of people economically inactive due to long-term sickness (16-64)
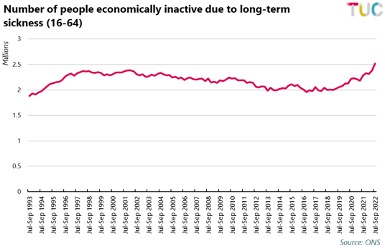
ONS data published in December 2022 72 highlighted that economic inactivity is rising ten times faster amongst people with self-reported Long Covid. Between July 2021 and July 2022, the inactivity rate amongst working-age people with Long Covid grew by 3.8 percentage points compared to 0.4 percentage points for working-age people without Long Covid. The ONS conclude that working-age people are less likely to be in the labour market after developing Long Covid than before catching Covid-19 and that Long Covid is likely to be one of the factors contributing to the declining levels of labour market participation.
The data also finds that people with self-reported Long Covid 18 to 29 weeks after a Covid-19 infection were more likely to experience long term absence compared with the time before they caught Covid-19.
There is a growing body of evidence on the impact of Long Covid on the labour market. For example, research in July 2022 73 estimated that current levels of Long Covid could be causing 110,000 workers to be missing from the labour market, and thus amounting to lost earnings of £1.5bn per year.
ONS data shows that the sectors most impacted are health, social care and education. However, the impact on other sectors should not be underestimated. Data shows the next sectors with the highest numbers of people with self-reported Long Covid are the civil service/local government, transport and retail.74
The evidence that Long Covid is contributing to people needing to take long periods of time off work or leaving the labour market altogether emphasises the need for government action to support people with Long Covid so they can stay in work should they wish to and be able to. This is vital should the government want to address rising economic inactivity, keep experienced staff in our public services and ensure that people are able to support themselves and loved ones. In addition, support for people who are no longer able to work is essential. There are structural and personal barriers to gaining employment and government support must recognise this to ensure people who can no longer work due to Long Covid live well.
The Public Sector Equality Duty means public authorities must have due regard to the need to achieve the objectives set out in the Equality Act 2010 to:
- eliminate discrimination, harassment, victimisation and any other conduct that is prohibited by or under the Equality Act 2010
- advance equality of opportunity between persons who share a relevant protected characteristic and persons who do not share it
- foster good relations between persons who share a relevant protected characteristic and persons who do not share it.
This applies to the government’s actions to tackle economic inactivity, especially given that certain groups such as women and disabled people are more likely to experience Long Covid.
Workplace transmission
There is growing data demonstrating exposure in the workplace has been a significant source of Covid-19 infection. There were 93,000 Covid-19 cases reported to enforcing authorities in 2020/21 which employers believed may have been caused by exposure at work with 64 per cent of all reports made by employers from the health and social care sector.
Since 1 April 2022 the only cases of Covid-19 which are reportable to HSE are due to either deliberately working with the virus (for example in a laboratory) or being incidentally exposed to the virus from working in environments where people are known to have Covid-19 (such as in health and social care). Cases due to general transmission (either worker-to-worker, or from contact with members of the public) are no longer reportable. Therefore, we no longer have accurate data on workplace transmission and due to under-reporting, acknowledged by the HSE, it is likely that thousands of cases of work-related Covid-19 have remained uncaptured.
However, available data does show that a correlation between certain occupations and Covid-19 exposure fatality. Data from the ONS indicates that workers in the food service sector, retail, health and transport are among those with the highest rates of death involving Covid-19.75 A recent study by the ONS76 points to jobs where social distancing and working from home were not possible as a factor to why infection rates were so high.
Due to high levels of workplace transmission the TUC and Long Covid Support have been calling for prescription of Covid-19 as an occupational disease. An occupational disease is an illness or a condition that can arise or be caused as the result of unsafe working conditions or exposure to certain substances in the workplace and if prescribed, individuals would be eligible for Industrial Injuries Disablement Benefit (IIDB). Long Covid must also be included in any prescription of Covid-19 as an occupational disease.
The Industrial Injuries Advisory Council (IIAC)77 has recommended prescription of a number of long-term symptoms associated with Covid-19; designating it an occupational disease for Health and Social Care Workers who have experienced five named complications.
We urge the government to accept the recommendation of the IIAC and in addition, to recognise Covid-19 as an occupational disease beyond health and social care and those five named complications. This would entitle more front-line workers to protection and compensation if they contracted the virus while working. We are also out of step with international practice; a report compiled by the International Labor Organization (ILO)78 detailed schemes by more than 50 states.
There has now been on case of a nurse successfully applying for IIDB after contracting Covid-19 from a patient as she was able to evidence that her Long Covid diagnoses was most likely the result of work-related activity.79 Having Covid as an occupational disease would reduce the burden on workers to take individual cases.
- 68 https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00299-6/fulltext
- 69 https://www.tuc.org.uk/research-analysis/reports/creating-healthy-labour-market
- 70 Ibid
- 71 https://www.bankofengland.co.uk/speech/2022/may/michael-saunders-speech-at-the-resolution-foundation-event and https://www.ons.gov.uk/employmentandlabourmarket/peoplenotinwork/economicinactivity/articles/halfamillionmorepeopleareoutofthelabourforcebecauseoflongtermsickness/2022-11-10#:~:text=Source%3A%20Office%20for%20National%20Statistics%20%E2%80%93%20Labour%20Force%20Survey,-Embed%20code&text=However%2C%20between%202019%20and%202022,172%2C000%20increase%20seen%20among%20women
- 72 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/selfreportedlongcovidandlabourmarketoutcomesuk2022/selfreportedlongcovidandlabourmarketoutcomesuk2022
- 73 https://ifs.org.uk/news/110000-workers-missing-work-result-long-covid-cost-ps15-billion-year-lost-earnings
- 74 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/alldatarelatingtoprevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk
- 75 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/bulletins/coronaviruscovid19relateddeathsbyoccupationbeforeandduringlockdownenglandandwales/deathsregisteredbetween9marchand30jun2020
- 76 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19infectionsinthecommunityinengland/characteristicsofpeopletestingpositiveforcovid19inengland22february2021
- 77 https://www.tuc.org.uk/news/ministers-must-not-abandon-workers-long-covid
- 78 https://www.ilo.org/wcmsp5/groups/public/---ed_emp/---emp_ent/documents/publication/wcms_741360.pdf
- 79 https://www.rcn.org.uk/magazines/Advice/2023/Jan/Long-COVID-benefits-support
The TUC and Long Covid Work conducted a self-selecting online survey. The survey was open from 14 September to 1 November 2022 and was promoted on social media, through affiliated unions and Long Covid support groups. We received 3,373 responses from people who self-reported they had Covid-19 and of these, 3,097 reported they had Long Covid. The analysis in this report is of respondents who reported they had Long Covid.
- 56 per cent of respondents with Long Covid are in full-time employment, 24 per cent in part time employment and eight per cent are unemployed.
- Eight per cent identified as BME and 90 per cent as White.
- 76 per cent of respondents are women, 21 per cent men and one per cent non-binary.
- Less than one per cent of respondents identified as trans and 98 per cent did not identify as trans.
- 35 per cent identified as disabled and 59 per cent did not identify as disabled.
- Nine per cent of respondents identified as lesbian, gay or bi and 83 per cent identified as heterosexual.
- 15 per cent of respondents are under the age of 35, 83 per cent between the ages of 36 and 65 and just under 2 per cent over the age of 65.
- The majority of respondents worked in education (33 per cent) or health and social work (28 per cent) and 64 per cent said they were a key worker.
- 45 per cent of respondents had caring responsibilities, of which 6 per cent cared for someone with Long Covid.
- The regions with the largest responses were as follows. 28 per cent of respondents were from London and the South East, 13 per cent were from Scotland and 12 per cent from the North West.
One limitation of this data set is the low levels of responses from certain sectors where we know Covid-19 infection was high; for example, transport (1 per cent of respondents) and retail (2.5 per cent of respondents). There was also a low response rate from self-employed people (3 per cent) or respondents on zero hours contracts (1 per cent).
Long Covid symptoms
Nearly all (92 per cent) of respondents who told us that they had Long Covid said they were currently experiencing symptoms. The most common symptom was fatigue with over nine in ten (96 per cent) respondents stating they had experienced this. The other most common symptoms were cognitive dysfunction – difficulty with thinking and concentration (84 per cent), shortness of breath or difficulty breathing (73 per cent), difficulty sleeping (65 per cent), cognitive dysfunction – memory loss (63 per cent), fast-beating or pounding heart (60 per cent), dizziness (57 per cent) and digestive problems (53 per cent).
Over half of respondents reported pain related symptoms including muscle pain (60 per cent), headaches (60 per cent), joint pain (58 per cent) and chest pain (50 per cent). Additionally, a significant number reported mental distress with half (50 per cent) reporting symptoms of anxiety, four in 10 (40 per cent) changes to their mood and over a third (37 per cent) depression.
A significant minority of respondents also said they had experienced pins and needles (44 per cent), tinnitus or earaches (41 per cent), a cough (38 per cent), sore throats (36 per cent), loss of problems with smell (34 per cent) and taste (30 per cent), dermatologic symptoms (31 per cent), problems with vision or eye health (30 per cent), higher temperature or intermittent fever (25 per cent).
Over two in 10 (23 per cent) respondents said they experienced lung function abnormalities, one in 10 (11 per cent) had experienced inflation of the heart muscles and just under one in 30 (2.5 per cent) had experienced acute kidney injury.
A quarter (25 per cent) of women and non-binary respondents reported that they had experienced changes to their menstruation. Graph II demonstrates the different symptoms experienced.
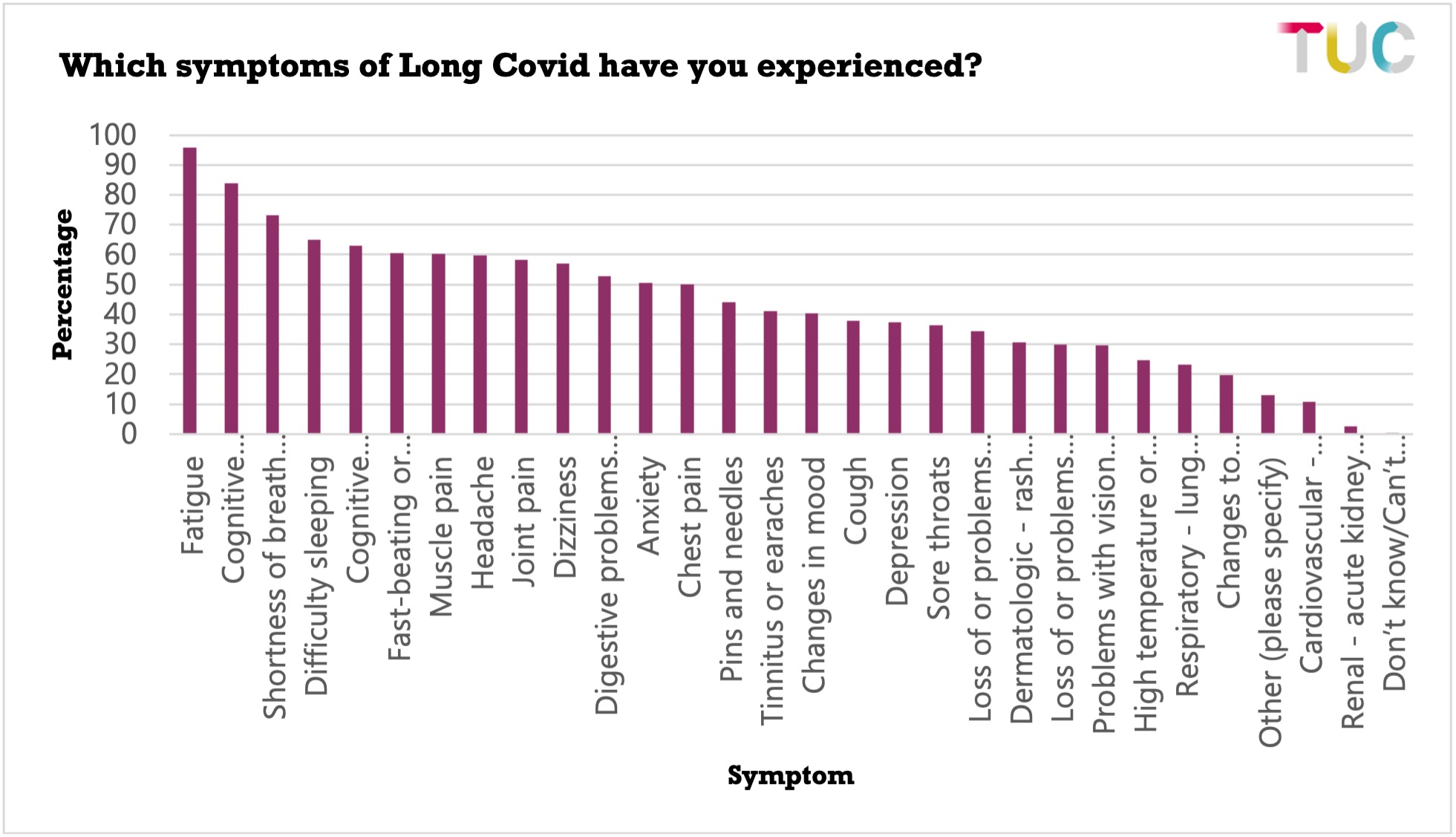
Respondents could select as many of the listed symptoms as was relevant to their experience of Long Covid. On average each respondent reported having 13 of the 29 Long Covid symptoms we asked about and described the severity of their cumulative impact.
This report focuses on the impact of work and therefore we will not provide a narrative of why people experience different symptoms or the pathology of Long Covid. However, collecting data on the symptoms contributes to the literature of people with Long Covid having a key role in identifying and defining what Long Covid is and how they experience it. It also highlights that people with Long Covid will need different support from their employer depending on the symptoms they are experiencing, highlighting the importance of believing and listening to the person.
Over nine in 10 (93 per cent) respondents also stated that their symptoms varied over time, for example they were worse on some days in comparison to others or affected them for part of the day. In the comments, many respondents stated that this was not well understood by their employer
“The fluctuating and relapsing/remitting nature of Long Covid was not accommodated well. Once I'd had my phased return that was it, I was expected to be well enough to work at full capacity.” Woman 46–55 Health and social care
“Long Covid is not linear. I was trying to overdo in my good days to compensate for the bad ones but it backfired. My director changed and he just used that fluctuation in performance to make me redundant.” Woman, 36–45, IT, communications, media and publishing
Additionally, over eight in 10 respondents (86 per cent) said they experienced post exertional malaise. This is the worsening of symptoms following physical or mental activity, which can mean that people have to limit their activities and need additional rest periods. Again, employer support needs to take these experiences into account.
Impact of symptoms
Respondents also told us how long they had been experiencing symptoms for and the impact their symptoms had on their ability to carry out day to day activities.
The most common length of time that respondents had been experiencing symptoms was over 24 months (29 per cent of respondents), followed by 7 to 12 months (23 per cent). In our survey in April and May 2021, the most common length of time was 3 to 6 months (35 per cent).
Overall, 60 per cent of respondents said they had been experiencing symptoms for over a year. This compares to 29 per cent in 2021.
Six in 10 respondents (63 per cent) told us that their ability to carry out normal day to day activities had been limited a lot and a further third (33 per cent) reported that their ability to carry out day to day activities had been limited to some extent.
Whether each person meets the Equality Act 2010 definition of disability would need to be based on the experiences of that individual, however, four in ten of all respondents reported both that their symptoms had lasted for 13 months or more and their ability to carry out normal day to day activities had been limited a lot. This suggests that many who responded to our survey would meet the required definition under the Equality Act 2010, meaning that if they had been denied reasonable adjustments, their employer could potentially be acting unlawfully.
Workplace transmission
There is evidence that the workplace has been a significant site of transmission. Half of respondents (49 per cent) to the survey said they had reason to believe they had contracted Covid-19 at work.
Almost two thirds (64 per cent) of all respondents identified as key workers, and of that group, six in 10 (61 per cent) had reason to believe that they contracted Covid-19 whilst at work. Several respondents described contracting Covid-19 at work, with some describing the inadequate safety measures which they felt had led to transmission and the additional layer of injustice that doing their job has led to the situation they are in.
“I am a secondary school teacher… I know I contracted Covid at work despite my own adherence to protections. I taught in a very crowded, poorly ventilated classroom. I love my job and don’t want to be off. Because I’d only been in the post for a year, I got one month full pay and one month half pay. It feels really unfair. I’m in this situation because I did my job.” Woman, 46–55, education
“I caught Covid in March 20 and think I caught it from the hospital I work at as later found out there was an outbreak of Covid and we had no PPE. I believe [employer] failed to protect me and failed in their duty of care as a vulnerable member of staff at high risk of Covid complications which I have suffered and am still severely unwell 31 months on.” Woman, 36–45, Health and social care
Reasonable adjustments at work
The survey asked questions about the support that individuals had asked for at work and what they had received from their employer. Getting reasonable adjustments from employers is not only important to inclusive working and preventing discrimination and negative treatment, but to ensure that work is not worsening someone's Long Covid symptoms.
Sharing symptoms
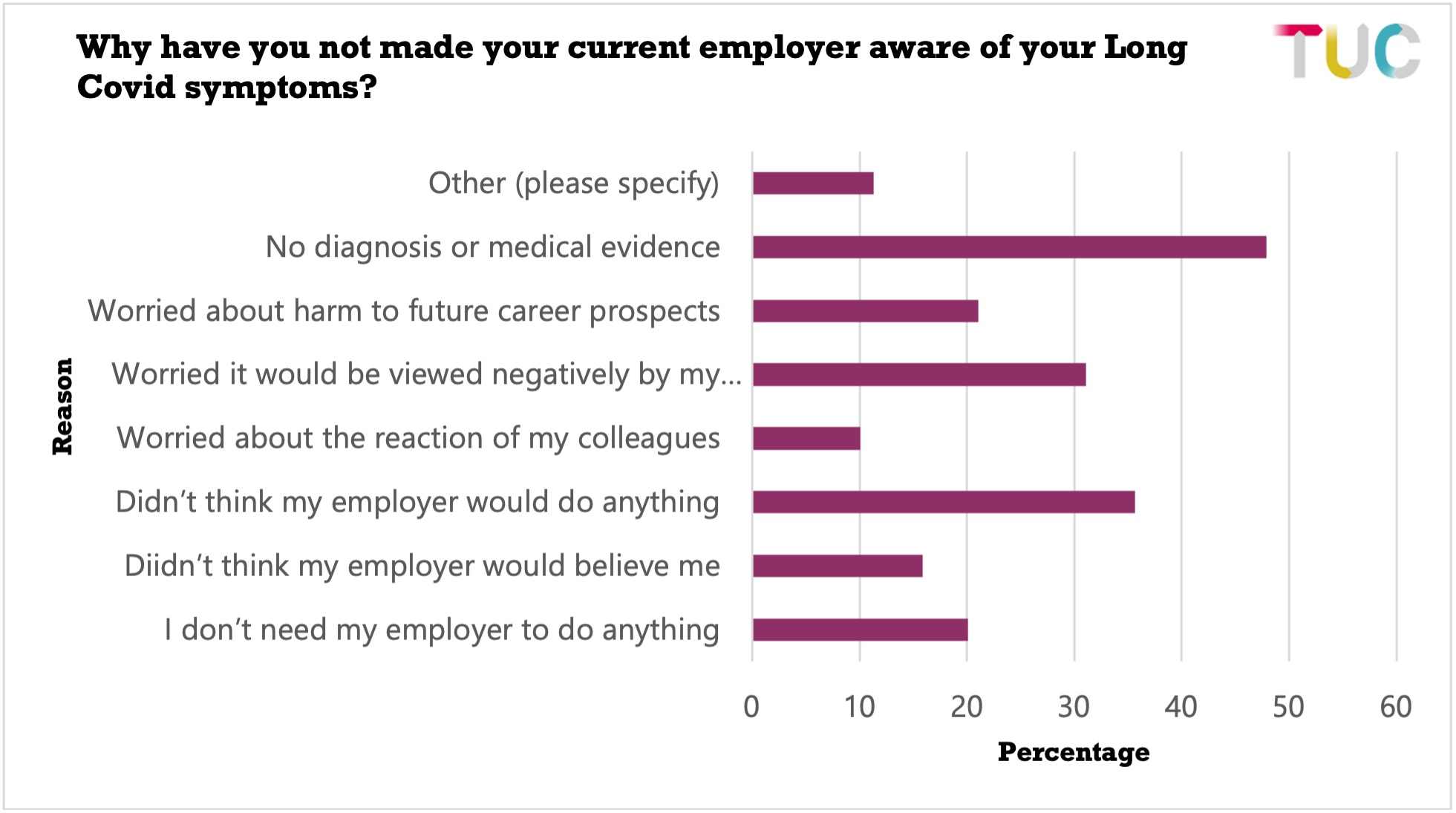
The majority (59 per cent) of respondents said they had made their employer aware of all their symptoms and just under a quarter (23 per cent) made their employer aware of some of the symptoms. However, one in eight (12 per cent) said they did not inform their employer of their Long Covid symptoms at all.
Almost half of the workers (48 per cent) who did not communicate their symptoms to their employer cite a lack of diagnosis or medical evidence — without these they thought they should not or could not raise the issue. This is concerning because, despite numerous symptoms identified by the World Health Organisation, Long Covid remains a diagnosis of exclusion and diagnosis frequently depends on numerous separate tests for other conditions which are difficult to get referred to and take a long time to obtain due to waiting lists stretching to months and sometimes beyond a year. In addition, a diagnosis is not needed to receive support from your employer but a combination of misinformation, stigma and common acceptance of the medical model of disability can leave workers feeling they need one in order to ‘prove’ their impairment.
Further, one in three (36 per cent) respondents said they didn’t think their employer would do anything or said they were worried that their symptoms would be viewed negatively by their employer (31 per cent). More than one in five (21 per cent) were worried about the potential harm that disclosing their symptoms would do to their career prospects and 16 per cent didn’t think their employer would believe them. Only one in five (20 per cent) said they hadn’t shared their symptoms because they didn’t need their employer to do anything.
Requesting adjustments
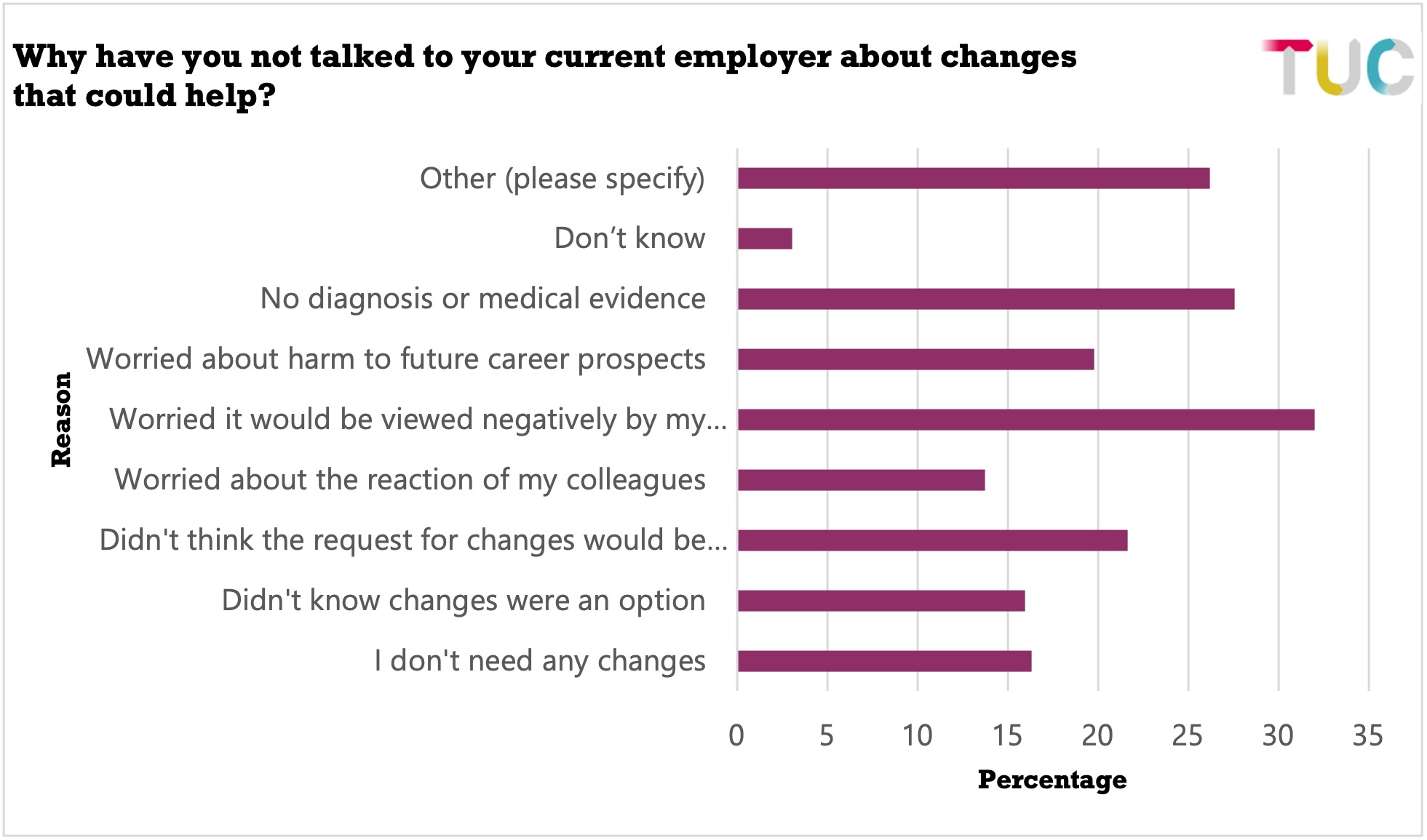
Of the respondents that had told their employer about their Long Covid symptoms, two in three (65 per cent) had requested changes that would help them manage their job or return to work. But worryingly, one third (33 per cent) had not.
Again, we see a pattern of fear of stigma and disbelief. Of the respondents that had not asked, only one in six (16 per cent) said it was because they did not need any changes. One in three (32 per cent) said they were worried that they would be viewed negatively by their employer. The other main factors were, again, lack of medical diagnosis (28 per cent) and thinking the changes would not be approved (22 per cent). Almost one in five worried that asking for changes would harm their career prospects (20 per cent). More than one in ten (15 per cent) didn’t know that changes were an option and 13 per cent were worried about the reaction of their colleagues.
Reasonable adjustments for returning to work
We asked respondents what adjustments they had asked for to support their return to work. Overall, one third (35 per cent) of respondents who asked for changes said their employer had made all the changes requested but worryingly, this is down from our report in 2021 where 44 per cent of respondents said all changes had been made.
And, concerningly four in ten (40 per cent) said only some of the changes were put in place (this was 31 per cent in 2021) and eight per cent said none of the changes (this is the same percentage as the 2021 survey) were made meaning that almost half of respondents were not given all or any of the changes they need to return to work. One in sixteen (six per cent) were still waiting for a response.
We asked respondents which changes they asked for and which their employers had put in place.
In two categories, phased return to work and support from occupational health, more respondents had a change implemented than asked for it. Just over half (54 per cent) of respondents asked for phased return to work and 65 per cent received a phased return to work. Similarly, 47 per cent of respondents asked for occupational health support and 55 per cent received it. This pattern was the same in our 2021 results.
In the case of phased return, almost 40 per cent of respondents who had a phased return to work reported that this was between four weeks and four months. The fact that more people had phased return to work implemented than asked for it indicates a tendency for employers to see phased return as the main solution, expecting the person with Long Covid to have a linear recovery and return to their healthy self at the end of it. The reality is different, as Long Covid recovery is not linear, and it is a fluctuating condition.80 Of the respondents who had taken time off, 42 per cent had been off for more than one period of time, which includes 10 per cent of respondents who reported making more than three attempts at returning to work – and being off again as their symptoms relapse. Only a third (32 per cent) were able to return to work on their first attempt.
Reassuringly, a quarter (26 per cent) of respondents said their current employer was “reasonably supportive” and allowed them time of work before returning. A further 23 per cent said their employer let them have as much time off work as they needed. However, 16 per cent said they had been pressured to return to work before they were ready.
Comments from respondents also expressed frustration at employers not understanding that symptoms would continue and fluctuate.
“Now I'm back, expectations are that I will cope. Impatience that I'm not getting better. Guilting from HoD (Head of Department) that I'm 'on the radar' as being paid full time and not lecturing. That I shouldn't go for promotion in case the university finds out. All very stressful.” Woman, 36–45, education
The percentage of respondents asking for a temporary change or reduction in hours and time off to attend a Long Covid clinic was the same as those that received it.
In all remaining categories fewer workers received a requested change than asked for it. Noticeably, four of the five changes with the biggest discrepancy between asked for and put in place are forms of flexibility - flexibility to support fluctuations in my symptoms, longer or more frequent breaks, permanent home working and other changes to my hours (see Table I for the figures). Additionally, fewer than half the number of people who asked for physical changes to their workplace to help them return to work (e.g., improved ventilation, lighting, seating, workstations) received those adjustments.
In our 2021 survey, flexibility to support fluctuations and longer/more frequent breaks were the most frequently asked for changes but also had the biggest discrepancy between being asked for and being put in place. Flexibility in different forms, but especially to manage fluctuating symptoms, that can be made beyond a phased return to work is a key adjustment for workers with Long Covid to be able to return to work but are more likely to be turned down by employers.
- 80 As covered under Guidance to the Equality Act.
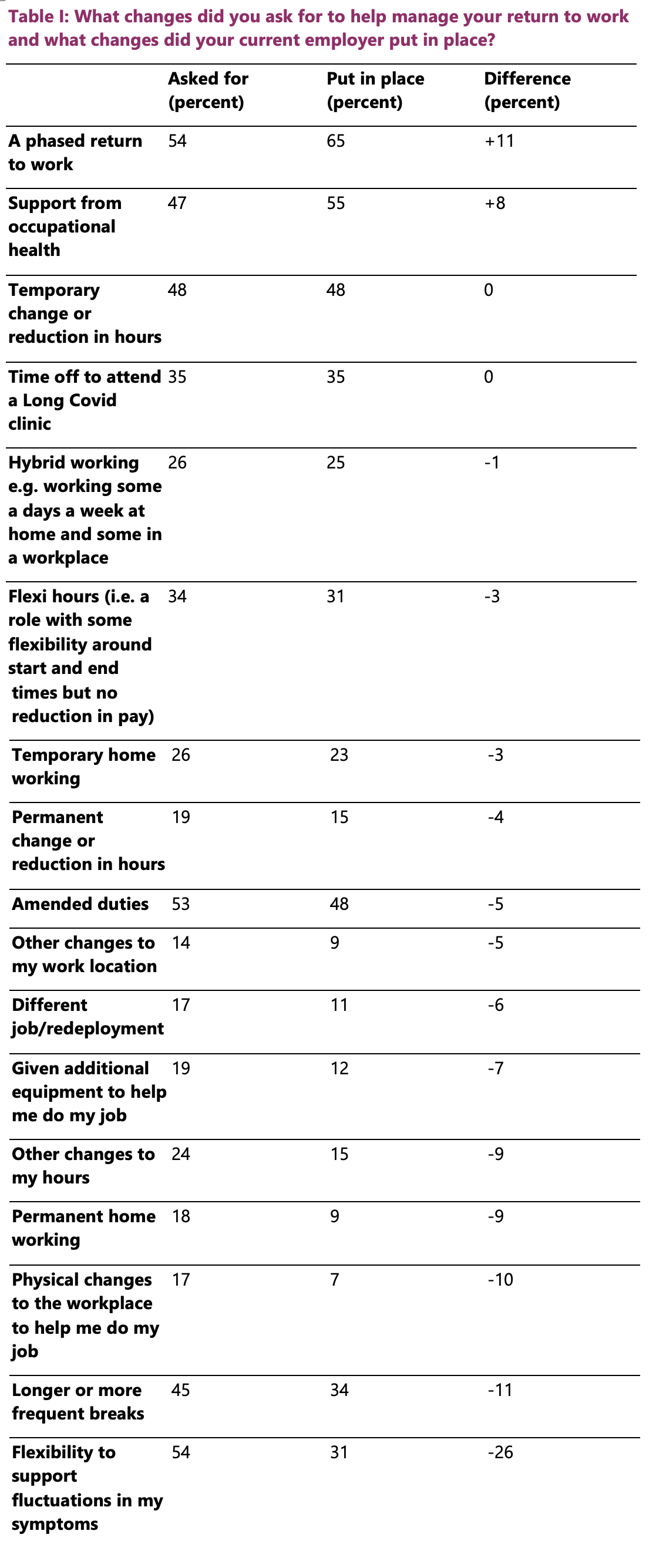
Reasonable adjustments to help manage work
We also asked respondents what changes they asked for to help them manage their job. Again, half of respondents were not given all or any of the changes they need to manage their job – 11 per cent had their changes rejected and 39 per cent only had some of their changes made. Just over one third (37 per cent) had all of the changes they asked for made to help them manage their job. One in sixteen (6 per cent) were still waiting for a response at the time of the survey.
We see similar patterns when looking at the changes to manage their jobs. More respondents had support from occupational health put in place than asked for it. And similarly, the most frequently asked for changes were amended duties, temporary changes or reduction to hours and flexibility to support fluctuating symptoms. However, again three of the five changes with the biggest discrepancy between asked for and put in place are forms of flexibility - flexibility to support fluctuations in my symptoms, longer or more frequent breaks and permanent home working (see Table II).
Employers' reluctance to offer forms of flexibility may reflect a combination of the stigma that we know exists towards flexible working, a lack of understanding at the fluctuating nature of Long Covid and a post-exertional malaise and disbelief from employers on what is needed by people experiencing symptoms.
Additionally, 20 per cent of respondents asked for additional equipment to help them do their job and only 11 per cent received this and only around half the number of requests to make physical changes to workplaces to enable the person with Long Covid to do their job were granted – including improvements to ventilation for workers with Long Covid who wanted to avoid repeated infections.81 This came across in the comments as well.
“FFP3 masks — asked for — been refused.” Man 26–35, health and social care.
“Asked for HEPA filtration, proper air ventilation and contact tracing within the office but all were refused. Was told air filters are too expensive by a company worth over £200million.” Man, 26–35, PR, advertising and market research.
“Asked for Health and Covid 19 risk assessment and ventilation in the office - no response. Also asked for ventilation and mitigation measures during meetings and all staff meetings - no response.” Woman, 26–35, Charity/Third Sector.
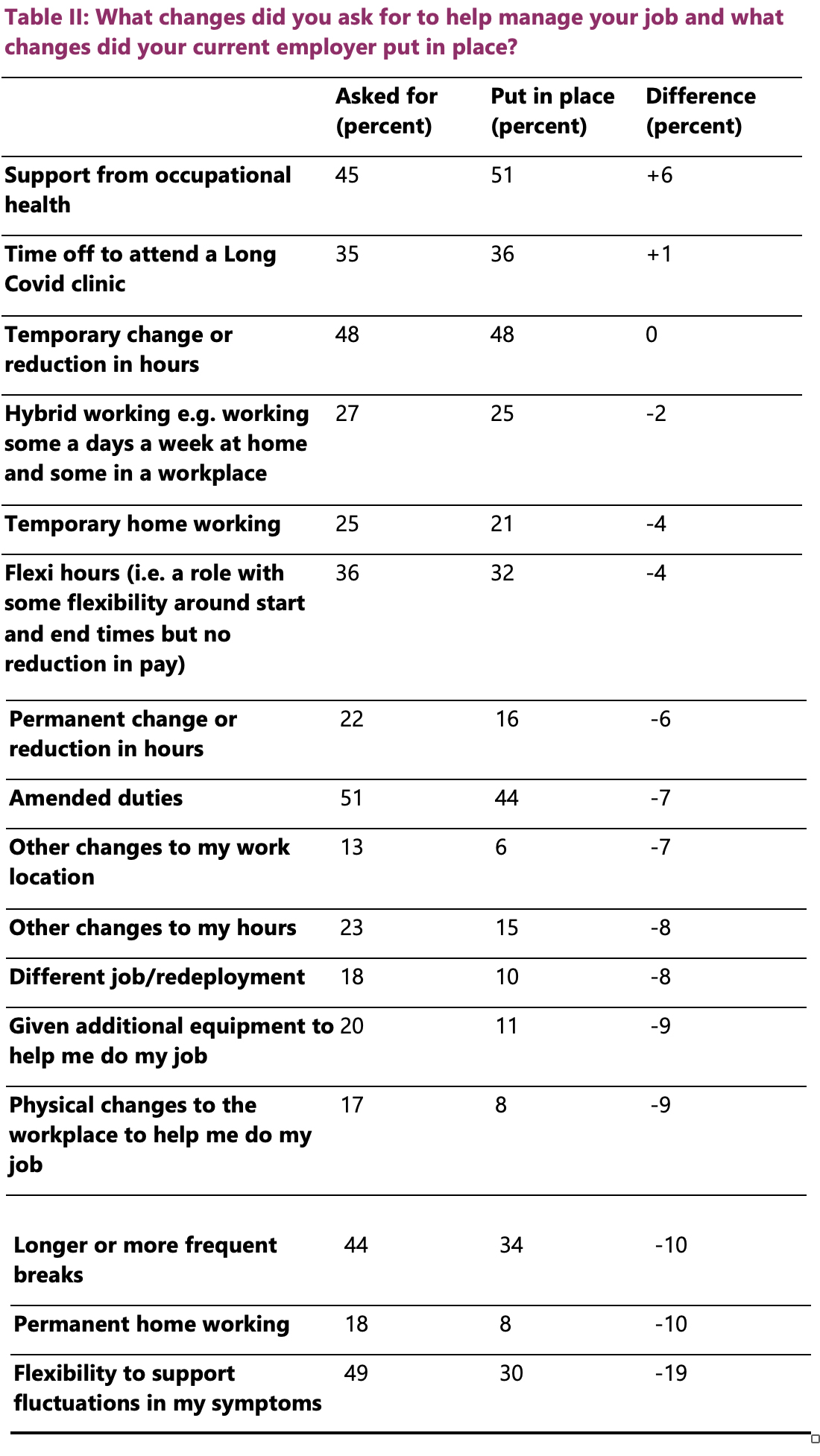
When comparing to 2021, the percentages of people asking for different changes has stayed largely consistent, other than there has been a slight jump in people asking for permanent change or reduction to hours from 15 per cent in 2021 to 22 per cent in 2022 and people asking for redeployment from 10 per cent in 2021 to 18 per cent in 2022. Some changes are not directly comparable.
Comments from respondents showed the serious impact a lack of, or poorly managed, adjustments had on their symptoms, demonstrating that bad employer practice can worsen people’s health and lead to relapse.
“Even though officially changes have been made, ongoing management and colleague pressures pushed me beyond my limits and I ended up relapsing fully, to the point that I’ve been off work for the past ten months.” Woman, 36–45, health and social care.
“I returned to work and built up a phased return to 5 hours a day over 5 months (all working from home). I was then overloaded with work so now been off sick for over a month due to a flare up in symptoms.” Woman, 26–35, legal.
“OH recommended permanent WFH. Senior manager disagreed, even when WFH national guidance in place. Stress caused from their trying to force issue, with other manager demanding.... WFH & office meant I relapsed with LC and have not been able to go back to work.” Non-binary, 46–55, health and social care
Barriers to reasonable adjustments
For the respondents who said they had not asked for certain changes to either return to work or manage their job we asked why they had not done so. The survey paints a complex picture of factors that preclude workers from asking for changes, including workers being uninformed about their rights.
More than 40 per cent of respondents who did not request specific changes, felt that those changes were not needed.
However, even if the worker would have benefited from changes, a quarter of respondents (25 per cent) did not request them because they did not know these changes were an option.
Other reasons cited for not requesting changes reflect a fear of request being rejected and damaging workplace relationships and career prospects.
- One third (32 per cent) said they did not think the request for changes would be approved.
- Three in ten (29 per cent) of respondents said they were worried that it would be negatively viewed by their employer.
- Two in ten (20 per cent) said they were worried about potential harm to future prospects.
- Just under two in ten (18 per cent) were worried about the reaction of their colleagues
Other reasons that respondents provided for not securing changes included waiting for approval, Occupational Health advice or equipment to be delivered or a failure by the employer to provide adequate staff coverage to accommodate the adjustment.
“There is no-one else who can take over my work duties if I don’t do them. So even though I had a reduction in work hours, the jobs I had to do were the same.” Woman, 36–45, Charity/Third Sector.
Treatment at work
To understand how Long Covid impacts experiences at work we asked respondents if they had experienced different types of unfair treatment. Respondents were able to select all the types of treatment they had experienced.
Our results show that the fear of negative consequences that precludes workers from speaking to their employer is well justified.
Responses demonstrate the enormous impact that having Long Covid can have on people’s experiences of work ranging from the impact on career progression to loss of hours and ultimately jobs.
Performance and progression
Almost three in 10 (28 per cent) respondents told us they were concerned Long Covid has affected their chances of a promotion in the future and 15 per cent told us their colleagues or manager have questioned their commitment to their job.
“Told not to go for promotion in case I draw attention to myself and my illness (even though we agree I meet the criteria for promotion).” Woman, 46–55, education.
Additionally, one in 20 (five per cent) said they had been denied training opportunities.
Disbelief
Almost a quarter of respondents (23 per cent) said their employer has questioned whether they have Long Covid and/or the impact of their symptoms.
“My boss questions my symptoms - said it seemed like a lot of symptoms for one person, as if I was lying.” Woman, 46–55, education.
“[My manager] does not fully understand the impact of LC and therefore has made comments which suggest she feels it is equivalent to her own tiredness etc and that I should therefore be able to ‘push through’.” Woman, 36–45, education.
This is similar to the disbelief that many with people energy-limiting impairments face in the workplace. More than 80 per cent of respondents to a survey done by Chronic Illness Inclusion felt that people think “everyone gets tired” and experienced this as disbelief of their experience82 .
Sick leave and management action
Sick leave was raised by a significant number of respondents with just over a quarter (27 per cent) of respondents stating that the amount of sick leave they had taken had triggered absence management or HR processes and over one in ten (13 per cent) told us they had used all of their sick leave entitlement and had been told there would be negative consequences if they took more.
To address the issues with sick leave, a common adjustment for disabled people is disability leave, which is a period of time off work which has been approved by an employer for a reason related to an employee’s impairment. This often means that the leave taken does not count towards sickness absence which may trigger a review or action by managers. However, one in 25 respondents (4 per cent) had been told they could not take disability leave.
One in 13 (8 per cent) told us they had been threatened with disciplinary action, while fewer (three per cent) had been subject to disciplinary action.
“Been subject to disciplinary action due to excessive breaks, was watched an[d] singled out, being watch on CCTV.” Woman, 36–45, wholesale and retail.
One in 15 (seven per cent) respondents had also been subject to capability proceedings.
“I have been told by OH that HR will seek to remove me on grounds of capability if I don’t come back to work soon.” Woman, 46-55, health and social work.
Loss of hours, job or pay
A number of respondents highlighted the impact having Long Covid had on their job security. One in seven (14 per cent) of respondents said they had:
- been forced to take early
- felt forced to resign to protect their health
- felt forced to leave their job for other Long Covid related reasons or;
- felt they had been singled out unfairly for redundancy.
“I was 55 yrs old when I was made redundant with Long covid symptoms and other disabilities. Since my redundancy, I have taken a much junior role not reflective of my skills, qualification and experience.” Woman, 56–65, education.
“Absolutely awful experience losing my job. They ignored the advice of the OT and instead went down the route of making me redundant. I was the only person in the whole organisation made redundant so it was definitely related to my health issues and my wanting reasonable adjustments which they couldn't justify not giving me.” Woman, 36–45, agriculture.
Additionally, respondents shared the impacts of Long Covid on hours worked, pay and terms and conditions. Seven per cent had been forced to take additional unpaid leave, four per cent had not received a pay rise/bonus when other colleagues had and five per cent had experienced negative changes to other benefits (e.g. their pension etc.).
“Impact on pension and earning bonuses as not fit to work so on half pay and unable to take extra shifts as could do when well.” Man, 36–45, Legal.
Conversely, over one in five respondents (22 per cent) told us they felt forced to work more hours than was good for their health because they needed the money.
“I feel that actually taking care of my health without losing pay or damaging any prospect is impossible.” Woman, 26–35, education.
“Because I had to reduce my working hours I have not been able to finish paying off my debts in order to retire. So I am still working despite having reached the age of 65 and feeling exhausted.” Woman, 36–45, education.
Treatment by managers and colleagues
One in six (16 per cent) respondents told us they had been subject to bullying and/ or harassment, for example being ignored or excluded, singled out for criticism or excessive monitoring of work.
“I have been the subject of jokes or comments about not being fit or healthy enough before Covid, being overweight, about Covid being created to get rid of people like me, being lazy, long Covid symptoms psychological and therefore my own fault, that it can't be that bad etc.” Woman, 26–35, Charity/third sector.
Respondents also told us of negative changes that had been made to their job:
- Seven per cent had been given simpler or more junior tasks at work compared to colleagues in a similar role/level of seniority
- Four per cent had been given harder or less popular tasks at work compared to other colleagues in a similar role/ level of seniority
One in seven respondents (14 per cent) also told us they had experienced other forms of negative treatment, examples of which are provided below.
“I can’t pass a job interview as the adjustments I have in place for my job with brain fog aren’t appropriate for interview.” Woman, 46–55, IT, communications, media and publishing.
“Unable to locum/take extra shifts (as not well enough) to supplement income which will affect maternity pay.” Woman, 26–35, health and social work.
“I have requested ill health retirement but declined as LC is a new condition so permanency cannot be determined.” Woman, 46–55, central government.
“I’ve had to use annual leave to reduce my hours each week.” Woman, 46–55, health and social work.
“I've had an offer to go onto a zero hours contract – I refused. Then after months, a phone call asking me if I'd like to resign – again I refused.” Woman, 56–65, health and social work.
Case studies
The importance of employers supporting workers with Long Covid cannot be overstated. Whilst Long Covid is not linear and people’s symptoms will fluctuate, supporting people means retaining skilled, capable and long serving staff and perceptions on reasonable adjustments need to be shifted to view them as something positive rather than challenges.
The two case studies on the next pages highlight some stories in more detail.
I caught Covid-19 while working on a Covid contact ward in October 2020 and I have been off work since. After 3 or 4 months, we were out of the acute stage. But both my husband and I were still off work as we were experiencing many of the classic symptoms of Long Covid – breathlessness, brain fog, and muscle and joint pain.
I’m about to start a 4-week phased return to work and I’m worried about that. I’m not sure 4 weeks is going to be enough after being so ill for two and a half years. Following Covid, I’m now deaf in one ear, I have blurred eyesight and a heart condition. I’m only 35 but I’m menopausal. And I’ve developed mass cell induced histamine. This means I have an intolerance to most foods, and I can come out in such severe allergic reactions that I have to carry an epi pen with me.
I think employers need to do much more to help staff with Long Covid stay in their jobs. I’m involved in advocacy work for people with Long Covid. People tell me they don’t feel supported and that not enough is being done to put measures in place to retain the workforce. People are either having to return to work wholly – or they’re giving up and leaving work entirely. There’s nothing in the middle.
I know of other nurses who are having to go to employment tribunals for not getting reasonable adjustments. That’s hard when you’ve devoted your whole career and your whole life to the health service. I had a meeting with our CEO and chief nurse over a year ago when I raised my concerns about the lack of support for people with Long Covid at work. We agreed an action plan – but now, some 14 months later, not a single action has been done. We need a step change and real action on Long Covid. People are suffering now. We can’t afford to ignore this any longer.
I work in the universities sector. I caught Covid-19 in March 2020. At the time there was nothing in place to deal with Long Covid problems and little understanding, particularly from my GP. I took two weeks off work following the infection and my employer was very understanding about this, it was during the first lockdown, and everyone was struggling.
At that point I thought I'd recover fully, but after limping on trying to recover for six weeks, while jiggling a shift to remote work and dealing with a young family, I was allowed to go on furlough. When I returned to work approximately two months later, around in summer 2020, I was still not better, and my boss agreed for me to work reduced hours.
Over time it became obvious that I wasn't the only one that was struggling to recover from a Covid-19 infection and as the numbers of Long Covid sufferers increased, my organisation developed some useful support materials and a support group that helps us meet people in the same situation and discuss how we're managing our symptoms.
We've had presentations on how to manage energy limiting conditions and advice on how to broach the subject with line managers. We've even had scientists and doctors give seminars on Long Covid.
It was only after approximately two years (with lots of ups and downs), I began to feel as if I could manage full time work again. Sadly, the system is not set up for such long recoveries and – long before I felt well enough – I had to force myself through many months of pushing too hard to the detriment of both my health and quality of work.
I suffered a reinfection in December 2022, which really knocked me back in terms of quality of life and how much I could work in a week. Fortunately, there is a much better understanding of the problems faced by Long Covid sufferers now, and both my GP and workplace have been more supportive and constructive in helping me return to work. However, there is still a misconception that recovery is just a matter of a couple of extra weeks rest and there seems to be only so much patience offered to people once they're over the acute infection.
All in all, I feel lucky that my organisation has been supportive and proactive in terms of helping people remain in work and balance recovery, or, adjusting to the new world of working with Long Covid. However, I fear that, although my organisation has put in place support for people with Long Covid, the societal shift hasn't yet happened. I feel wary of sharing that I have Long Covid and still try to hide symptoms as I fear that I will get a reputation as being unreliable or lazy. I feel a lot more could be done in educating the wider workforce.
Non-social security financial support
We asked respondents if they received any financial support excluding Department for Work and Pensions’ (DWP) support.
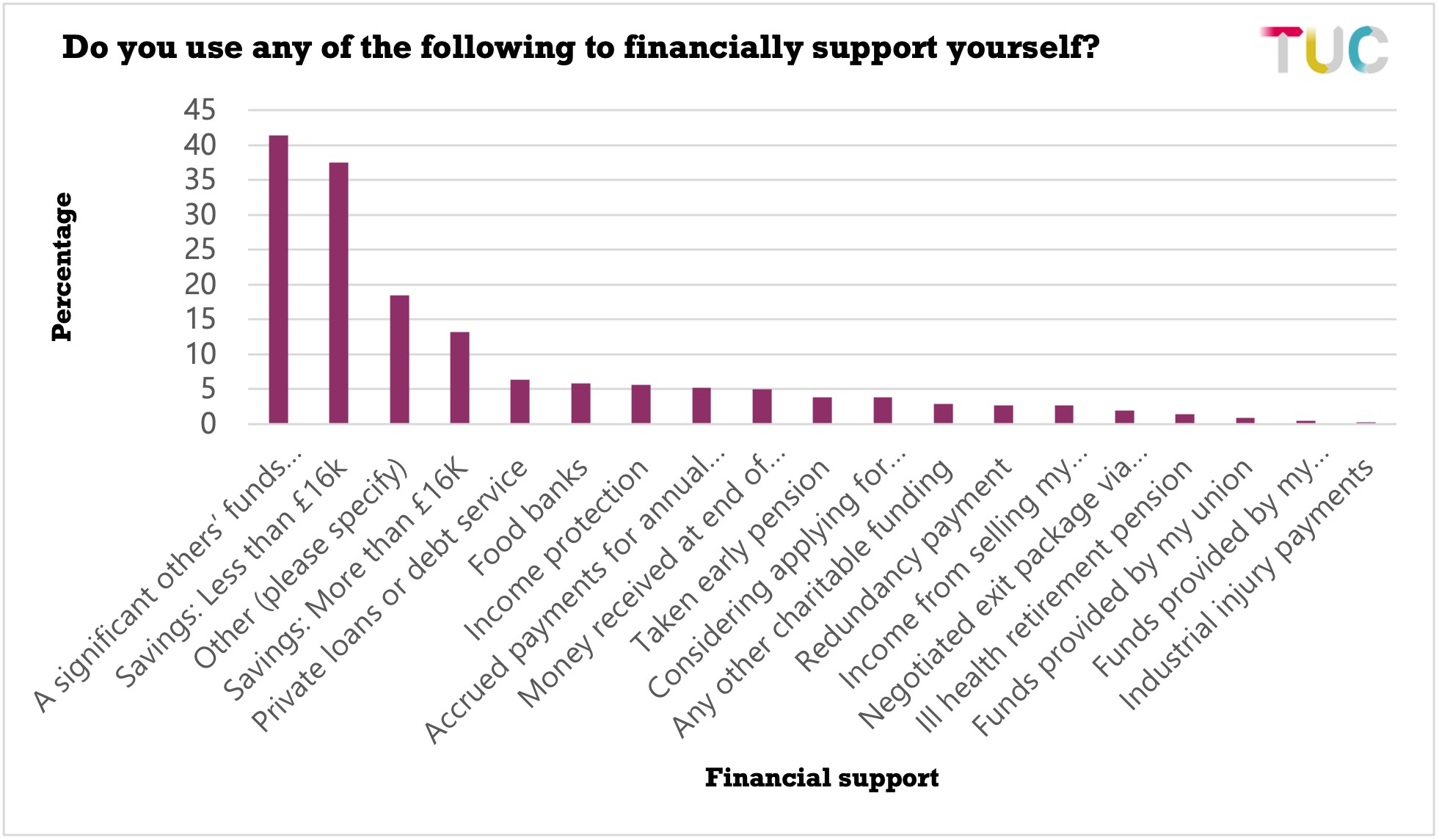
The most common form of financial support reported by respondents was their savings (50 per cent), of which 38 per cent had savings of less than £16,000 followed by four in ten respondents (41 per cent) who relied on a significant others’ funds (e.g., partner, parents, friends).
It is worrying that people with Long Covid are having to rely on savings to financially support themselves and even more concerningly the percentage taking out private loans or using a debt service e.g., pay day loans, loan sharks (6 per cent) with a further (4 per cent) having considered applying for a private loan or debt service. Additionally, one in sixteen (6 per cent) told us that they were using food banks.
Some respondents reported receiving financial support on leaving their job which included:
- money received at the end of employment (5 per cent)
- accrued payments for annual leave (5 per cent)
- a redundancy payment (3 per cent).
The comments provided by respondents revealed that some people felt they were just about surviving on their current level of income:
“So far I am surviving on half pay as I now get PIP. My money runs out in December. Then I will have no income.” Woman, 36–45, education.
While other respondents talked about having to find ways to both save expenditure and bring income into the household, worryingly sometimes through increased debt and risky forms of financial support.
“Maxed out credit cards, overdraft, money from friends, selling possessions, food voucher from council, not buying food, limiting energy use.” Woman, 56–65, other sector.
“Moved to cheaper housing / region to cope with lower income - now hours away from workplace.” Woman, 46-55, education.
“Renewed my mortgage to pay debt off.” Woman, 46–55, health and social care.
“Overdraft and credit card.” Woman, 65+, other sector.
The selling of personal possessions reported by respondents also included items such as “jewellery”, “cars”, and a “motorbike”.
Concerns and uncertainty about how any future income could be secured was evident especially when employment related sick pay was close to ending:
“Currently receiving full pay on NHS sick leave but will lose my job if unable to return in January so will likely have to sell my house.” Woman, 46–55, health and social care.
“None so far but currently planning to downsize our house to manage financially.” Woman, 36–45, Charity/third sector.
Other forms of financial support that were shared which included Statutory Sick Pay, special leave, child benefit, funds by professional bodies, charitable funding, funds provided by their union and taking early pension which could lead to financial uncertainty in the future.
Department for Work and Pensions support
In addition to the financial support reported above, we asked respondents whether they currently received any support from the Department for Work and Pensions (DWP).
Most of the respondents (78 per cent) reported they were not in receipt of state support and (19 per cent) reported they were. Just over a third of respondents who stated they were in receipt of benefits (38 per cent) stated they received employment support allowance (ESA)83
and three in ten received Universal Credit (30 per cent). Almost six in
Other forms of income reported by respondents included: the state pension, war pension, tax credits, Disability Living Allowance, child benefit (this respondent did not claim it previously) and child tax credits.
The comments on people’s experiences about applying for DWP support showed two key themes. Most of these responses detailed negative experiences of applying for social security with only ten of 334 responses being positive.
- Challenges with the DWP processes
- Worsening of health and wellbeing.
- Challenges with the DWP processes
There were a number of barriers in this section including uncertainty on eligibility for certain support and the difficulty with the application process. Many respondents who had applied for one or more benefits reported the DWP’s claims process to be “very lengthy”, “confusing”, “complicated”, and “very hard work”. Consequently, it is perhaps unsurprising that common ways in which these respondents described their experiences of the DWP as a “nightmare”, “horrendous”, “horrible” and “appalling” and for one respondent to conclude it was “unfit for purpose”.
Respondents talked about how hard it was to complete the required paperwork for a claim especially when they experienced cognitive dysfunction and or fatigue. As these two respondents put it:
“Difficult and confusing form and process. Especially for someone with cognitive and fatigue issues. Took me two weeks to fill the form. If I hadn't got help from benefits and work website I wouldn't have got the benefit.” Woman, 46–55, other sector.
“PIP and ESA questionnaire drained my energy and took me a long time…” Woman, 36–45, education.
“Extremely difficult when you have cognitive issues. I have currently given up contesting as I'm in the wrong PIP group.” Woman, 46–55, education.
Respondents reported that their time scales for completing the required paperwork ranged from two weeks to two months. It was common for respondents to seek support for such tasks too. For example, from their partner, friends, family members and or third sector assistance: “I had help from Citizens Advice completing the forms.” Sometimes the need to seek support led to delays in submitting a claim. In addition, respondents referred to the length of the process including any appeals.
Challenges with the process also applied to appeals. Some respondents told us how they had to battle and endure lengthy mandatory reconsiderations or appeals which could extend a time scale of up to 16 months to be awarded a benefit:
“First application 6 months in resulted in not eligible, went through reconsideration but still not eligible. Reapplied 16 months later and was awarded pip all very stressful.” Woman, 56–65, health and social care.
However, some told us that they felt unable to appeal given how difficult the process is and the effort required.
“I found it a degrading experience. The report was farcical, and I decided not to appeal to get mobility benefit as it would take too much energy.” Woman, 36–45, health and social care.
- Worsening of health and wellbeing
Respondents talked about numerous negative health and wellbeing impacts that they associated with making a DWP claim. Overall, the process was commonly reported to be “very very stressful” by many of the respondents.
In addition to stress, there were many other significant negative health related impacts reported by most of the respondents’ both physical and mental which they attributed to undertaking the application process. For example, many respondents talked about the worsening and exacerbation of their ill-health and Long Covid symptoms, with some experiencing a significant ‘’crash” that lasted for a prolonged period as well post exertional symptom exacerbation after making a claim.
“All of this process is incredibly stressful and exhausting and has a detrimental effect on long covered symptoms especially when only advice from GP is to rest.” Woman, 36–45, charity/third sector
Regardless of whether financial support was provided or not, respondents often described their experiences of claiming as “demeaning”, “dehumanising”, “degrading”, humiliating and talked about being left with a range of emotions and traumatic type feelings. Some respondents explained they were made to “feel like you're lying” “made to feel like a cheat for trying to claim PIP” or “guilt”.
“I was made to feel like a criminal rather than a ill person holding on by their fingernails they in the process have worsened my condition and I have not yet over a year later regained the already tiny baseline that I lost as a result of this.” Woman, 36–45, other sector.
Very worryingly, two respondents reported suicidal ideation.
“What a nightmare system almost ended my life trying to access this for disability is impossible.” Woman, 36–45, education.
These responses highlight the degree of variability of experiences people may have when claiming social security. However, the significant negative health impacts often over a prolonged period of time is a significant concern that needs to be addressed.
This also demonstrates the need for Covid-19 to be recognised as an occupational disease and therefore for people to be able to apply for IIDB, to ease the process for receiving financial support and for people with Long Covid to be given clear and accurate information on what they should do.
- 83 30 per cent stated they were in the support group and seven per cent in the work-related group.
In the survey we also asked about people’s current employment status; seven per cent (214 people) of people told us they were currently unemployed and had lost their job since March 2020. Whilst the sample size is small, we feel it is important to recognise the unique experiences of this group.
Of them, almost nine in 10 (88 per cent) believed they had lost their job due to Long Covid and half (53 per cent) had reason to believe they had contracted Covid-19 at work.
When looking at the symptoms they experienced, the most common were, as with other respondents, fatigue (98 per cent compared to 96 per cent overall), cognitive dysfunction – difficult with thinking and concentrating (95 per cent compared to 84 per cent overall) and shortness of breath or difficulty breathing (84 per cent compared to 73 per cent overall).
They were more likely to report certain symptoms and more likely to report a range of other symptoms for example, fast-beating or pounding heart (80 per cent compared to 60 per cent overall), dizziness (76 per cent compared to 57 per cent overall), cognitive dysfunction – memory loss (74 per cent compared to 63 per cent overall), headaches (74 per cent compared to 60 per cent overall), joint pain (71 per cent compared with 58 per cent overall), chest pain (70 per cent compared to 50 per cent overall), lung function abnormalities (35 per cent compared with 20 per cent) and inflamed heart muscles (20 per cent compared to 10 per cent overall).
Additionally, they were more likely to have experienced symptoms for longer periods of time – almost half (48 per cent) had experienced symptoms for over 24 months compared to 29 per cent of all respondents. Overall, 84 per cent of unemployed respondents had Long Covid for over 12 months. Shockingly, but perhaps not surprisingly, nine in ten of respondents out of work said their ability to carry out normal daily activities had been limited a lot.
When looking at their experiences of work:
- A third (34 per cent) said they felt forced to resign to protect their health.
- A third (32 per cent) said that the amount of sick leave they had taken had triggered an absence management or HR process.
- Almost three in 10 (28 per cent) said they felt forced to leave their jobs due to other Long Covid related reasons.
Of the respondents who had been become unemployed since March 2020, half (54 per cent) said they were using a significant others’ funds to financially support themselves, four in 10 (40 per cent) said they were using savings of less than £16,000.
Some of the quotes provided by respondents out of work recognised how unfair it was that they had caught Covid-19 at work with life changing consequences.
“I gave everything, including my health to teaching. I wish I hadn't. My employers did everything to support me during my contract, knowing it would end and they could replace me. I blame lack of funding from the government forcing schools to make cutthroat decisions. My employer, in effect is the government. They should declare that front line workers who caught covid get a compensation payment.” Woman, 4–-55, education.
“I caught covid at work because my employer failed to adapt and take appropriate infection prevention measures. I was the only employee to be furloughed two weeks after I was signed off and they sent notice of redundancy by post without any conversation or consultation.” Woman, 36–45, legal.
“I caught Covid-19 at work in March 2020 after I was sent on a business trip that I believe should never have gone ahead [leading to a] life-changing and life-limiting disability as a result.” Women, under 26, wholesale and retail.
Stay Updated
Want to hear about our latest news and blogs?
Sign up now to get it straight to your inbox