‘Health is Everyone’s Business’
The TUC welcomes the opportunity to contribute to the DWP and DHSC consultation on health and job loss. The TUC’s affiliates have extensive experience relating to health at work, offering their members advice and support where health has an impact on their working lives. This ranges from support offered by union reps in the workplace, to legal advice and support from union officials and legal officers.
As a result, trade unions have much of value to contribute to this consultation and we hope that if implemented in the correct way, these proposals for reform will improve the world of work for all.
Summary of recommendations:
- Government proposals on health in the workplace should focus on prevention first. Trade unions have a long record of promoting health and safety in the workplace. We believe all unions should have a right of access to workplaces and that the government and employers should promote and support strong trade unions
- Government should introduce a right to workplace modifications (rather than a ‘right to request’).
- No-one should be too low paid to qualify for sick pay. The lower earnings threshold for qualification for Statutory Sick Pay should be removed. Waiting days for statutory sick pay should also be abolished.
- Government should focus on investing in occupational health capacity within the NHS, rather than encouraging employers to invest in private provision.
- The government should make the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) a part of UK law enforceable in UK courts
It is important to view these proposals in the context of the existing provisions relating to health in the workplace. A decade of austerity has taken its toll. Wide ranging cuts to public services and state funded provisions relating to workplace health, as well as large scale contracting out of services, has resulted in significant failures in the duty of both government and employers to protect workers’ health.
In our affiliates’ experience, examples of current failings in the system include the fit note scheme, the disability confident programme, Access to Work and occupational health provisions. And all of this is against the background of an NHS suffering from years of cutbacks, outsourcing and reorganisation.
Not only have there been major gaps in resourcing, but also there are fundamental problems with culture in the workplace and how employers perceive disability, ill health and other conditions affecting workplace performance.
Our affiliates experience widespread complacency amongst employers in this respect and report consistent failures by employers to comply with the duty to implement reasonable adjustments for disabled people under the Equality Act 2010.
We also know there are significant problems with the statutory sick pay system. In particular, many people who are in low paid, insecure work currently miss out on SSP, despite being the most in need.
In addition, many employers are failing in their duty to protect the health, safety and welfare at work of employees and others.
For some employers, this is due to lack of awareness of their responsibilities and their compliance needs to be nurtured, built, reinforced and monitored.
However, some employers deliberately evade their legal duties. These employers need to be identified and enforcement action taken against them. Their business practices are harmful to workers and serve to allow them to under-cut responsible employers in the same sector.
Against this background, we emphasise that in order to be successful, any measures proposed in this consultation must be adequately resourced, implemented and enforced and backed up by a fully resourced and supported NHS.
Key proposals for supporting health at work
- Prevention first
We believe that the focus of any measures intended to reduce ill health related job loss must be the prevention of work-related ill health and sickness absence.
Many adults of working age have chronic health problems that are the result of their previous or ongoing experience at work. Unless this particular cause of ill health is addressed, the problem of ill health related job loss cannot be resolved.
Government statistics report that 1.4 million workers in the UK were suffering from work-related ill health in 2017/18.The rate of long-term ill health caused by work has been increasing since 20111 . In 2017/18 stress, depression or anxiety accounted for 44 per cent of all work-related ill health cases and 57 per cent of all working days lost due to ill health2 . These figures illustrate the shocking extent of the problem and just how much action is required to address this.
We also emphasise that early intervention is key to reducing ill health related job loss. Some workers may require modifications and support at work, but have not yet had any or significant periods of sick leave. Failure of employers to assist at an early stage, for example, by failing to promptly implement reasonable adjustments, may serve to exacerbate health conditions and lead to sickness absence and ultimately job loss.
- The right to request modifications
Whilst we greatly welcome the proposal for a new right to request workplace modifications, our preferred outcome would be for a “right to have” workplace modifications, rather than a “right to request”.
The existing process for making a request for flexible working under the Flexible Working Regulations 2014 has served to highlight the difficulties with employment rights systems based on a right to request only. We are strongly of the view that any such flaws must be avoided in relation to this new proposal.
We also highlight the importance of ensuring that the new proposals do not interfere with or undermine the duty to implement reasonable adjustments under the Equality Act 2010, or any existing maternity-related entitlements.
How the reforms are implemented is fundamental to their level of effectiveness. We recommend a technical consultation to ensure exiting rights are not undermined and that there is a seamless flow between the operation of the new proposals and the existing reasonable adjustments regime under the Equality Act 2010.
In terms of eligibility for this right, we argue for as broad an application as possible, extending the right to all workers, and assert that the right should not be dependent on a period of sick leave.
When considering the extent of the duty, we also encourage a focus on the social model of disability, as opposed to the medicalised approach. We are strongly against any length of sickness absence being a requirement for eligibility. This is on the basis that it is not only those people with conditions resulting in sickness absence who may require workplace modifications.
- Statutory sick pay
The SSP qualifying rules require significant modification to ensure broad and fair coverage. To this end, we recommend the removal of “qualifying” and “waiting” days and that SSP is an entitlement from day one of employment.
We also strongly support the removal of the Lower Earnings Limit (“LEL”) threshold. At the moment, LEL excludes large numbers of workers from SSP entitlement. In particular, those who are in irregular and insecure work, such as zero hours contracts, and women who are in low paid work. We do not accept that this widened entitlement should only be given at a reduced % SSP, it should be paid in full.
Current enforcement of SSP is ineffective and we encourage the adoption of an enforcement model based on that used for the National Minimum Wage.
We support increases in both the amount and length of sick pay. As well as benefitting workers, this may well incentivise employers to focus on prevention and rehabilitation.
- Occupational health
We welcome the recognition by the government of the importance of the Occupational Health (OH) services, the massive and increasing deficiency of OH capacity and the lack of access to OH through employers.
We also strongly support the need to respond to the transforming labour market, and the commitment expressed to the principle of keeping workers safe, healthy and productive, and able to work if they wish to, despite having a chronic illness.
However, this consultation on the future of OH services available to employers and workers has several fundamental weaknesses that will undermine the impact of policy change and programmes that arise from it.
More than a million workers active in the labour market in the UK today have chronic health conditions that were caused at work. And there are very many people who are no-longer active in the labour market because of the impact of a chronic health problem that was caused by, or worsened at, work. The priority, if we are seeking to minimise exclusion from the labour market of people with chronic health problems is to stop making people ill through work.
There is also a great depth of displacement exhibited by very many employers; ‘this is not my problem, it is an external problem that the worker is bringing in to my workplace, I should not have to deal with this, and I cannot afford either the cost or the time in seeking to do so’.
It is vital to recognise the importance of the critical role of the NHS in the provision of OH services to employers, as a beacon for high standards and a primary source for new OH capacity. The questions in the consultation document do not address the long-term under investment in NHS OH capacity, nor its importance to building new capacity fit for the future.
The consultation document expresses the ‘government’s aspiration to see more employers purchasing OH through the private market’. We question the rationale for this. The aspiration should be for more employers to buy high quality and value for money OH services, from the public sector, third sector, or the private sector.
The existing and potential role of trade unions in the dialogue about, and management of, OH services in workplaces that are successful in this arena should be recognised.
- Advice and guidance
Whilst we are broadly supportive of additional measures to improve advice and guidance for employers, we wish to emphasise the importance of effective enforcement of statutory rights.
We also highlight the vital and unique role that trade unions play in ensuring that not only individual, but also collective health issues are addressed at work. Unions are uniquely placed to identify where there may be a collective health issue, such as stress due to widespread workplace issues, and to work with employers and employees to resolve this.
Union reps also play a crucial role in providing individual support and guidance. For example, helping employees negotiate reasonable adjustments at work.
Finally, strong collective bargaining is the foundation to a healthy workplace. We believe all unions should have a right of access to workplaces and that the government and employers should promote and support strong trade unions.
Q1. Do you agree that, in addition to government support, there is a role for employers to support employees with health conditions, who are not already covered by disability legislation, to support them to stay in work?
While the TUC strongly agrees that employers have a role supporting employees with health conditions, in our view employers have a duty to support a wider group of people than this question suggests. All workers, not only employees, should benefit from this support (please see question 4). Employers also have a duty to act to prevent the development of health conditions from the outset.
Employers should take active steps to prevent work related health conditions from developing. For example, preventing mental ill health linked to excessive workload. Where health conditions have already developed, employers should remove and reduce any barriers that disadvantage workers and could prevent those who are able to and who want to from staying in work.
The appropriate framework for these proposals is the social model of disability. However, the proposals put forward in this consultation appear to consider workers who are disabled people, or workers who have health conditions and are not covered by disability legislation, through the medical, rather than social, model of disability.
Indeed, the Equality Act 2010 definition of disability is predicated on the medical model and as a result focuses on a worker’s disability, impairment or health condition and frames them as a problem that needs to be fixed.
A new duty would be better served by the social model of disability, which focuses on the ways in which society is organised and the social and institutional barriers which restrict all disabled people’s opportunities. This model sees the person first and argues that the barriers they face, in combination with their impairments or conditions, are what disables them, barring them from full participation and meeting their potential.
The barriers identified in the social model are what make it impossible or very difficult to access jobs, buildings or services. The social model acknowledges the biggest barriers as people’s attitudes to disabled people.
In addition to framing the new duty within the social model, the government should, alongside this consultation, make the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) a part of UK law enforceable in UK courts. This would enshrine the social model of disability into law and make sure it informed policies affecting disabled people across the UK.
This would have an additional benefit for the UK government in that it would be a step towards full adoption of the UNCRPD Committees 2017 recommendations.
While the TUC welcomes any proposals that increase and enhance workers’ rights, we would not want any legislation that is developed because of these proposals to keep workers within the workplace for longer then they themselves want to work.
We also wish to highlight the importance of government support for individuals with health conditions, and the failure of current provisions, not least as a result of a decade of cuts to social security and public services. In addition existing schemes such as Disability Confident have failed in their objectives to improve conditions at work for disabled people. Disabled people need a decent social security safety net and in many instances for work to be structured differently, support given, and barriers removed.
Q2. Why do you think employers might not provide support to employees with health conditions not already covered by disability legislation to help them stay in work?
The duty to make reasonable adjustments has been enshrined in law for almost a quarter of a century, since the introduction of the Disability Discrimination Act 1995. And yet TUC research has found that one of the most common issues faced by workplace reps is disability-related issues. Over half of reps dealt with such issues between 2014 and 2016. These issues included ensuring employers put in place reasonable adjustments for their disabled workers as required by the Equality Act 2010.
Our research confirms the consultation’s assertion in para 36 that, ‘Some employers do not fully understand, or are unaware of, their legal responsibilities, for example, making reasonable adjustments for disabled employees or payment of sick pay.’ Our experience is that problems linked to putting in place reasonable adjustments are not just confined to smaller employers with limited resources but are experienced in organisations of all sizes.
In addition, our members’ experiences show that, as well as many employers not fully understanding or being aware of their legal duties to put in respect of reasonable adjustments, some intentionally discriminate against disabled people. This discrimination occurs at all stages of the employment life cycle, including recruitment, retention and promotion.
With employer practice being so poor in relation to disabled people who have had the protection of legislation for over a quarter of a century, it is not surprising employers have not taken adequate steps to support employees with health conditions where they are not protected under the law.
A cultural change to the way employers think about and act towards disabled workers and those with long-term health conditions is needed. Employers need to be encouraged to adopt an approach which focuses on the steps they need to take to remove barriers to full workplace participation rather than one that demands proof for the medicalised model of disability currently enshrined in law.
Q3. Do you agree that a new ‘right to request work(place) modifications’ on health grounds could be an effective way to help employees to receive adjustments to help them stay in work?
Yes.
The TUC welcomes government proposals to introduce a new right to request workplace modifications, but the level of effectiveness will depend on the scope of the right and how this is implemented.
Although the government proposals are very welcome, we support a “right to have”, rather than a “right to request” modifications
- Context
The TUC strongly supports the right of all workers to have a fulfilling, rewarding and happy working life. By the same token, it is important to highlight that staying in work will not necessarily always be the best outcome for all workers.
For those who do wish to stay in work the new right, if implemented in the correct way, could help prevent ill health, reduce periods of sick leave, and extend and improve working lives.
There are many problems with existing provisions for workers suffering from ill health and disability. For example, unions report to the TUC that the duty to implement reasonable adjustments under the Equality Act 2010 is rarely effectively implemented. Many workers do not necessarily qualify for the right to reasonable adjustments under the Equality Act 2010 but would nonetheless greatly benefit from workplace modifications.
We hope that a new and broader right to request workplace modifications will result in a change in workplace cultures, there employers become more receptive to carrying out workplace modifications, including supporting compliance with the right to reasonable adjustments provided for in the Equality Act.
- Right to have, not right to request
Although the government proposals are very welcome, we support a “right to have”, rather than a “right to request” modifications.
- Technical consultation
We recommend that the government carries out a technical consultation to clarify how these proposals will be implemented.
Should the government proceed with these proposals, they must do so in a way that ensures that existing rights are not in any way undermined. For example, existing rights of disabled people to reasonable adjustments, and existing maternity-related provisions.
This includes an employer's duty to make reasonable adjustments to a pregnant employee’s working conditions or hours of work in order to remove any health and safety risks and if the risks cannot be avoided 3 , the duty to offer suitable alternative work or provide a maternity suspension. It is vital the new modifications duty is clear the legislation that exists to protect pregnant employees has been maintained and steps are taken to avoid confusion of this legislative protection with the new duty.
Workplace modifications provisions should be formulated to strengthen and inform the existing duty to implement reasonable adjustments. Clear guidance must be given with distinctions drawn between the new duty and the right to reasonable adjustments to ensure both employers and workers are clear on their rights and their extent. It will be important these distinctions are supported with examples for clarification.
It is vital that flaws in the implementation of the Flexible Working Regulations 2014 (the Regulations”), are avoided when implementing the proposed right to request workplace modifications.
Recent TUC research has shown that around 3 in 10 requests for flexible working are turned down, with the current criteria that employers can use to justify this being so broadly drafted that employers have almost free reign to reject requests. Our analysis has found that as a result, the ‘right to request’ has failed to achieve the desired cultural change in workplaces, with a range of groups, including younger workers and parents losing out.
There have also been problems in relation to eligibility, a lack of the ability to scrutinise and challenge refusals, a lack of a clear formal right to appeal and a wide range of circumstances in which employers can reject requests. Limits on the number of requests allowed in a given period and the lack of a right to be accompanied by a trade union representative to meetings have also had a negative impact on the right to request flexible working process.
These are all issues which must be given consideration when looking at effective implementation of the new workplace modifications proposal.
A technical consultation should also review what type of modifications an employer will be required to undertake and the extent of the duty. The TUC considers that analysis of the modifications requirements should be based on the social model of disability, as outlined above.
This consultation does not address how the proposals will be enforced and what sanctions should be attached to breaches of any new duty. This is another aspect we suggest is included in a technical consultation.
In unions’ experience, reliance on individual enforcement alone is ineffective and places unacceptable burdens (in terms of cost, time and stress) on individuals. A statutory body must also have responsibility for enforcement and must be properly resourced to deliver on this.
- 3Management of Health and Safety at Work Regulations 1999, regs 16 – 18
Q4. If the government were to implement this new right to request work(place) modifications, who should be eligible?
- Any employee returning to work after a period of long-term sickness absence of four or more weeks;
- Any employee with a cumulative total of 4+ weeks sickness absence in a 12-month period;
- Any employee returning to work after any period of sickness absence;
- Any employee who is able to demonstrate a need for a work(place) modification on health grounds;
- Other, please state.
Workers should have the right to request workplace modifications without the need for a period of absence. No period of sickness should be required to trigger the new right.
In addition, eligibility for the right to request modifications should not be dependent on employee status. All workers should have access to this right regardless of their employment status - whether they have a contract of employment or similar contract for services. This includes but is not limited to the genuinely self-employed, freelancers or those employed on a short-term basis such as musicians, actors or comedians, and volunteers and interns.
The length of a worker’s period of sickness absence is not necessarily an indicator of the severity of the illness, condition or impairment a worker has or the extent of workers’ need for work (place) modifications.
One day off work for a reason related to a mental health condition, for example, could require steps are taken to ensure that barriers to participation in the workplace are addressed. A longer period of sickness absence, for example, because of a bout of chicken pox contracted later in life, could conceivably require few or no steps to be taken.
There are also workers who have not had a period of sickness absence from work, but would benefit from taking advantage of a new right to work (place) modifications.
Making work(place) modification before a period of sickness absence occurs is preferable to waiting for even one day of this type of absence that could be prevented by early intervention. There should be no qualifying sickness period for the new duty to activate. However, the practical steps an employer should take could vary depending on if a worker has been absent and the length of time taken.
The new duty should be based on the social model of disability, which would move it away from the requirement to ‘demonstrate a need for a work (place) modification on health grounds’ towards considerations about how to remove the barriers preventing full workplace participation and stopping workers from meeting their full potential.
Q5. How long do you think an employer would need to consider and respond formally to a statutory request for a work(place) modification?
- 0-4 weeks;
- 5-8 weeks; or
- 9-12 weeks?
We are of the view that 0-4 weeks would be an appropriate range of time for a response. The faster the response, the more likely that any measures will be effective. A long wait for a response and any modifications can impact negatively on a worker’s physical and mental health.
Unions have reported to us their experiences of the negative effect of extended delay in employer responses to requests to implement reasonable adjustments under the Equality Act 2010. We propose that if a short fixed period for a response is agreed in relation to a right to request workplace modifications, the same fixed time for a response should be applied in relation to the duty to implement reasonable adjustments.
Q6. Do you think that it is reasonable to expect all employers:
- To consider requests made under a new ‘right to request’ work (place) modifications?
Yes
- To provide a written response setting out their decision to the employee?
Yes
Q7. Please identify what you would consider to be legitimate business reasons for an employer to refuse a new right to request for a work(place) modification made on health grounds:
- The extent of an employer’s financial or other resources;
- The extent of physical change required to be made by an employer to their business premises in order to accommodate a request;
- The extent to which it would impact on productivity;
- Other – please state.
- Please give further views in support of your response.
As outlined above, we believe that a new right to request workplace modifications could work in a number of different ways and that a further technical consultation is required to properly address this.
We reiterate that it is important that careful consideration is given to how the new right to request modifications will interact with the existing right to request reasonable adjustments and that existing rights are strengthened, rather than undermined.
We believe that, if the government proceeds with a right to request, it must avoid the difficulties encountered with the right to request flexible working. Our research found that one in three requests for flexible working are being and that those in working class jobs were most likely to miss out on flexible working arrangements. 4 This highlights the reality that flexible working requests are easily and frequently turned down.
To ensure the same issues are not encountered the grounds for refusing a request to workplace modifications must be limited and highly defined.
Q8. The government thinks there is a case for strengthened statutory guidance that prompts employers to demonstrate that they have taken early, sustained and proportionate action to support employees return to work. Do you agree?
Yes – no – maybe – don’t know
Yes. We agree that there is a need for strengthened statutory guidance and that this should be introduced to support the new duty. We are however concerned that employers may find working with two distinctly different systems difficult and problematic. Under these proposals employers will have a duty to make reasonable adjustments for disabled workers and this new duty to make work(place) modifications (both of which look at adjustments to workplace functions).
It is imperative the new duty does not weaken, or create confusion about, the existing duty to make reasonable adjustments, and that it brings new rights for disabled workers rather than weakening their existing protections
This is why statutory guidance produced for the new duty should be clear on how the two duties interact with one another. The guidance would benefit from clearly structured with worked through examples to help avoid confusion and support compliance.
In addition, any changes must not only be made in legislation but must also be underpinned by a statutory code of practice, which clearly details all the steps an employer must take to comply with the new duty.
It is also possible workers will move from the protections under one duty to the other and so clarity on what rights and protections workers have under each and how they interact with each other will be essential.
Q9. If no, please give reasons for your answer.
n/a
Q10. If yes, would principle-based guidance provide employers with sufficient clarity on their obligations, or should guidance set out more specific actions for employers to take?
- Principle-based guidance provides employers with sufficient clarity;
- Guidance should set out more specific actions for employers to take;
- Don ’ t know;
- Other – please state.
We think that principles based guidance with illustrative examples would be of most assistance. The government should produce guidance that sets out the broad principles of the new duty to help with employer understanding. And, as highlighted above, any guidance must be underpinned by a statutory code of practice, which clearly details all the steps an employer must take to comply with the new duty.
This should be accompanied by scenario-based examples, which could examine, for example:
- how to remove different workplace barriers
- typical modifications and their associated costs
- what steps an employer would need to take where a worker, with a workplace modification, then required reasonable adjustments
This would aid employers by giving them a starting point on how to think about workplace modifications and then providing clear steps on how to comply, rooted in real life workplace situations. The guidance must also recognise the important role trade unions play in working with employers to ensure they comply with the law so workers' rights are delivered, negotiating and agreeing workplace policies, in raising and resolving disputes and working to create a positive working environment.
Q11. The government seeks views from employers, legal professionals and others as to what may be the most effective ways in which an employer could demonstrate that they had taken – or sought to take – early, sustained and proportionate action to help an employee return to work. For example, this could be a note of a conversation, or a formal write-up.
n/a
Q12. As an employer, what support would you need to meet a legal requirement to provide early, sustained and proportionate support to help an employee to stay in work or return to work from a long-term sickness absence?
- Better quality employer information and guidance;
- More easily accessible employer information and guidance;
- Easier access to quality OH services; or
- Other – please state.
n/a
Q13. As an employee: in your experience, what actions has your employer taken to support your health at work? Please describe how these were effective or ineffective.
The trade union backed “reasonable adjustments passport” is an example of a successful scheme, which has supported health at work. This could also be used in relation to the new right to request modifications.
The process was initially developed by a member of the Communications Workers Union (CWU) at BT, and has gone on to be widely used ensuring both the worker and their manager have a copy of that agreement.
A reasonable adjustments passport is a live record of adjustments agreed between a worker and their manager to support them at work because of a health condition, impairment or disability. It supports employers to ensure that up-to-date, appropriate, practical and correct reasonable adjustments are in place.
The passporting system means that workers who move roles, or find that their line manager changes, do not have to re-explain or renegotiate their reasonable adjustments.
The TUC and GMB have created a reasonable adjustment template, based in the social model of disability, which could be easily adapted to capture workplace modifications and is free to access by following the below link.
Q14. As an employee: what further support/adjustments would you have liked to receive from your employer?
Trade unions have extensive evidence of working with employers and employees to ensure that support is in place.
Royal Collage of Midwives (RCM) Reported Good Practice
The RCM has a number of examples of good examples where members have had reasonable adjustments put in place and have been supported fairly and compassionately, allowing employees to stay in work and the NHS to retain experienced staff.
One example was where a midwife with recurrent severe anxiety was unable to work shifts on a labour ward was supported to move to work in a clinic and later in a clerical role (with pay protection). Her employer also supported her to keep up their midwifery registration and she is now working as a midwife in another NHS trust.
Another example was where a midwife attempted suicide. She was given an extended return to work, was supported by a mentor and was supernumerary (e.g. not counted in workforce figures). Eventually, she was redeployed to a teaching role elsewhere in the NHS trust but has now been able to return to her original role.
Q15. All respondents: in order for employers to provide effective return to work support, what action is needed by employees? Select all that apply.
- To have discussions with their employer to identify barriers preventing a return to work and to inform workplace support;
- To agree a plan with their employer to guide the return to work process;
- To engage with OH services; or
- Other – please state.
We suggest that appropriate employee steps are set out in the statutory guidance and code of practice, finalised after consultation with trade unions and other stakeholders.
The TUC believes that active communication between employees and employers is essential and trade union involvement is central to this. However, we do not consider that active engagement with occupational health should be a requirement in all cases, particularly as the right to request modifications should, as outlined above, be broad enough to extend beyond health-based scenarios.
Examples of steps the employer could take include;
- have discussions with their employee to identify barriers preventing a return to work and to inform workplace support;
- agree a plan with their employer to guide their return to work process or the implementation of the work(place) modifications
- engage with OH services to identify additional barriers and ways to address them
Q16. All respondents: do you think the current SSP system works to prompt employers to support an employee’s return to work?
Yes – no – maybe – don’t know. Please give reasons for your answer.
No.
The TUC’s view is that the current SSP system does not adequately support employers to support an employee’s return to work.
While there is the requirement to provide SSP to eligible workers, what services employers make available to employees with health problems is determined by employers themselves.
Evidence shows that early intervention and sustained workplace support during sickness absence is important. 5 Effective absence management is about supporting employees with health issues to stay in or return to work
Statutory guidance needs to be strengthened for employees to encourage early intervention to support a sick employee to return to work.
Employers need to provide good management and training skills for their managers to allow them to do this. Some employees feel management have no time or the appropriate skills to deal with sickness absence.
Simple steps can be taken to ensure a swifter return to work. This includes a phased or gradual return to work, working the hours and days that would suit the employee. The design of SSP needs to be amended to accommodate a phased return to work, currently it is inflexible.
[5] https://www.ippr.org/read/working-well-a-plan-to-reduce-long-term-sickness-absence#
Q17. All respondents: what support would make it easier to provide phased returns to work during a period of sickness absence?
- Guidance on how to implement a good phased return to work;
- A legal framework for a phased return to work which includes rules on how it should be agreed and implemented;
- Clearer medical or professional information on whether a phased return to work is appropriate; or
- Other suggestions.
We refer to our answers above.
Q18. All respondents: would the removal of rules requiring identification of specific qualifying days help simplify SSP eligibility?
Yes – no – maybe – don’t know. Please give reasons for your answer.
Yes.
The rules around waiting and qualifying days in accessing SSP can be complex to understand, especially for those in insecure work who do not work set days and hours. The rules also reduce financial entitlement, as you have to be off sick a certain amount of days before receiving a payment.
Currently SSP is not paid for the first three days (waiting days), it is paid from the fourth day (qualifying day). The qualifying day is used by the employer to work out the days the employee can get SSP. Qualifying days are usually the employee’s contracted working days and hours. For example, if you are sick from Monday to Friday, and you normally work from Monday to Friday, you would receive just two days' SSP that week (for Thursday and Friday).
While for those working set days and hours it can be relatively straightforward in working out when entitlement begins, for those whose days and hours vary it can become very complex for the employer and employee to work out. To add to this issue, people in insecure employment face much more difficulty enforcing their rights. A lack of job security means that many people are afraid of raising workplace issues, as they fear losing their job. With rising forms of insecure work with unpredictable schedules, the TUC are concerned that workers may not be receiving their correct entitlement.
The TUC argue not only for the removal of rules around qualifying days but also waiting days. Three unpaid days of absence causes financial difficulties, especially for low paid workers, who often have to budget on a week-to-week basis. And workers will be forced to come in to work when they are not fit for work and this could cause longer-term health issues.
While it may be claimed that in- work universal credit claimants will be compensated for income loss, the design of universal credit results in a considerable delay in payments because of how the assessment period works. And there are many low paid workers not claiming universal credit as they are not eligible.
Q19. Do you agree that SSP should be extended to include employees earning below the LEL?
Yes – no – maybe – don’t know. Please give reasons for your response.
Yes.
It simply cannot be right that you can be considered too low paid to fall ill. The TUC believes that low-paid workers should have equal rights to SSP, paid at the normal rate, or at a rate equivalent to their normal weekly earnings if that is lower.
Currently those in work earning less than the Lower Earnings Limit (LEL) of £118 do not qualify for SSP or any financial support from their employer.
Removing the LEL hurdle would potentially extend SSP protection to around 2 million low paid employees. And TUC analysis shows this will predominately benefit women, as they are more likely to be low paid. Of the 2 million who will gain by removing this income threshold, 70 percent will be women. TUC analysis shows currently one in ten women employees are not entitled to SSP due do the LEL threshold. 6
The required earning threshold for SSP also means that those who are in insecure forms of work are also more likely to miss out on SSP. This is because their irregular hours may not result in them earning enough to meet the income threshold. TUC analysis reports there around 1.8 million employees in insecure work. 7 So those in insecure jobs may force themselves in to work even if they are unwell – putting their clients’ or fellow workers’ health at risk.
TUC analysis shows almost a quarter (23 percent) of those on zero-hour contracts do not meet the earnings threshold compared to 6 percent of permanent employees. 8
While this consultation does not say anything about a change in employee contributions for those earning under the LEL threshold, the TUC would like to make clear our objection to any change in contributions from those earning less than £118. These workers are already on low pay and if they have to pay NI contributions this would have a huge impact on their finances. A number of options should be explored to ensure that low paid workers do not have to make this trade off.
We do believe however, that measures should be taken to prevent employers from employing workers on a short hours basis to avoid paying employer national insurance contributions. The Office for Tax Simplification has previously recommended national insurance be levied on an employers’ whole payroll, rather than on the earnings of individual employees, reducing the financial incentive to offer work on a short-hours basis. 9 This could be one of the options to explore.
Q20. All respondents: for employees earning less than the LEL, would payment of SSP at 80% of earnings strike the right balance between support for employees and avoiding the risk of creating a disincentive to return to work?
Yes – no – maybe – don’t know. Please give reasons for your answer.
No.
The TUC believes that low-paid workers should have equal rights to SSP, paid at the normal rate, or at a rate equivalent to their normal weekly earnings if that is lower.
Anyone earning below £118 is on low pay and only receiving 80% of earnings when off sick will inevitably cause financial difficulties.
Workers need to take off appropriate time to make a more effective return to work and should not be financially threatened to return to work. It is also wrong to assume that at the full rate for sick pay you have no incentive to return to work. Sickness absence is not out of control, the latest figures for 2017 show sickness absence has fallen to the lowest rate on record. The figures show that employees took an average of 4.1 sickness absence days in 2017. 10 (Though there has not been an equivalent fall in the number of sickness-related welfare claimants – i.e. equivalent of ESA).
Rather than focusing entirely on incentivising employees the focus should be on incentivising the employer to ensure they have a good return to work plan for their workforce.
Q21. Do you agree that rights to SSP should be accrued over time?
Yes – no – maybe – don’t know. Please give reasons for your response.
No.
The TUC are opposed to the idea that rights to SSP should be accrued over time, as this would unfairly reduce entitlement to sick pay. People do not choose when to be sick,
In addition, those in insecure work would face the risk of never accruing sufficient entitlement when moving from job to job, making them financially more vulnerable.
All workers should have an entitlement to statutory sick pay from day 1 in their jobs.
Q22. Should the government take a more robust approach to fining employers who fail to meet their SSP obligations?
Yes – no – maybe – don’t know. Please give reasons for your answer.
Yes.
There needs to be a deterrent to stop employers avoiding their SSP obligations. Unfortunately, this can sometimes be the only way to ensure effective enforcement.
In the current system where employers fail to pay within the 30 – day appeal period, or after a tribunal hearing providing a final decision on liability, the employer can be fined up to £3,000 for non-payment of outstanding SSP.
This amount does not act as a deterrent and a stronger penalty is required. As discussed below the enforcement model of the NMW should be looked at for SSP.
Q23. Do you think that the enforcement approach for SSP should mirror National Minimum Wage enforcement?
Yes – no – maybe – don’t know. Please give reasons for your answer.
Yes.
The TUC position on the single enforcement agency is clear – we do not believe the creation of a single enforcement agency should be the priority for improving labour market enforcement. The scale and nature of non-compliance in the labour market is staggering and is a constant reminder of the need to increase the resources of enforcement agencies. The creation of a single enforcement body could end up being a costly, inwardly focused merger, which distracts from the important day-to-day enforcement work that is needed to address the significant noncompliance in the labour market.
Currently the enforcement regime for the NMW provides a stark contrast with the current arrangements for SSP and should be used as a model for improving how the latter is enforced.
The HMRC SSP disputes process is listed on GOV.UK however is not promoted more widely. They only deal with individual disputes to help employees get their legal entitlement and do not carry out more proactive work. It does not have the powers or resources to conduct targeted inspections of employers, or raise awareness among employers or employees.
The NMW model provides two routes. First, workers can take cases to Employment Tribunal, often with the help of their trade unions. Second, HMRC proactively enforce the NMW, taking a risk-based approach that allows them to focus on high-risk employers, occupations, industries and locales, as well as making some use of tax credit application data. This proactive enforcement is additional to HMRC’s commitment to investigate all first-party complaints received (e.g. those, made by named workers or their agents). This work is supported by a budget that is big enough to allow significant advertising and dissemination and by an enforcement staff numbering more than 500.
This has been successful, as HMRC recovered nearly £20 million of NMW underpayment for low paid workers last year. NMW enforcement has teeth, in terms of civil penalties for employers who fail to comply, plus a few prosecutions for the most serious cases. Clearly, this model has produced far more substantial results than the reactive approach used for SSP.
Our view is that SSP is a vital safety net for workers who are facing loss of earnings through ill health. Sufficient budget should be allocated to allow the HMRC to undertake proactive enforcement to supplement their “on-complaint” work. The agency should also develop a risk-based approach that would facilitate targeting the hidden non-compliance where no complaint has been received.
We also believe employers need to inform employees of their rights, as there can be a lack of clarity on eligibility to sick pay, particularly around the issue of employment status.
In 2017, the TUC carried out an online survey of insecure workers. A large number of respondents worked in the hospitality sector. Lack of awareness of the right to statutory sick pay was prevalent. Despite being eligible for statutory sick pay, many workers were not aware of this right and would not receive any pay whilst off sick. Furthermore, many respondents reported that they were fearful of taking sick leave as repercussions could include losing an assignment or future paid work.11
ACAS research from 2014 and 2015, shows that zero hours contract workers and agency workers are often unaware of their employment rights and afraid of raising workplace concerns due to fears over job security.12
We welcome the decision from the Government to bring forward legislation to make access to a day one written statement a right for both employees and workers, which will include details of eligibility for sick leave and pay.
- 4https://www.tuc.org.uk/news/one-three-flexible-working-requests-turned-down-tuc-poll-reveals
- 5https://www.ippr.org/read/working-well-a-plan-to-reduce-long-term-sickness-absence#
- 6https://www.tuc.org.uk/news/1-10-women-dont-earn-enough-qualify-sick-pay-tuc-analysis-reveals
- 7https://www.tuc.org.uk/research-analysis/reports/insecure-work
- 8https://www.tuc.org.uk/news/1-10-women-dont-earn-enough-qualify-sick-pay-tuc-analysis-reveals
- 9https://assets.publishing.service.gov.uk/government/uploads/system/uplo…
- 10https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/employmentandemployeetypes/articles/sicknessabsencefallstothelowestratein24years/2018-07-30
- 11https://www.tuc.org.uk/sites/default/files/TUCresponsetoTaylorreviewenf…
- 12https://www.acas.org.uk/index.aspx?articleid=5234
Q24. Do you support the SSP1 form being given to employees four weeks before the end of SSP to help inform them of their options?
Yes – no – maybe – don’t know. Please give reasons for your answer.
No.
A discussion between employer and employee needs to happen before four weeks of SSP ending. Regular contact needs to be maintained between both partners to ensure appropriate discussions of returning to work take place, and the SSP1 form needs to be issued earlier allowing more time for discussion and planning of the employee’s plans.
The employer should also provide guidance on Employment Support Allowance, if the employee is no longer entitled to sick pay.
Q25. All respondents: how could a rebate of SSP be designed to help employers manage sickness absence effectively and support their employees to return to work?
Open question.
The cost of SSP can be more difficult to manage for small and medium businesses. A small business could be in the unfortunate position of having eight staff with three off sick at one time. Smaller businesses require a rebate, as they should not be out of business through no fault of their own. The rebate also needs to be swift as smaller businesses often operate on smaller budgets.
At the same time however, there does need to be an incentive for smaller businesses to have an incentive to ensure they have adequate return to work plans/support for their employees. The rebate should only apply if the employer can demonstrate good practice, as outlined earlier in the consultation. A robust framework is required.
Q26. All respondents: at this stage, there are no plans to change the rate or length of SSP. The government is interested in views on the impact of the rate and length of SSP on employer and employee behaviour and decisions.
SSP is currently paid a flat rate of £94.25 a week for a maximum of 28 weeks. The income replacement level is around 20% and is amongst the lowest of its European counterparts, though the duration is longer. 13 While international models are more generous and may prevent sharp falls in income, the time period they apply to tend to be shorter than in the UK, and so may not provide sufficient support to those who have a longer recovery.
Sickness benefit replacement levels, EU 28, 2015 14
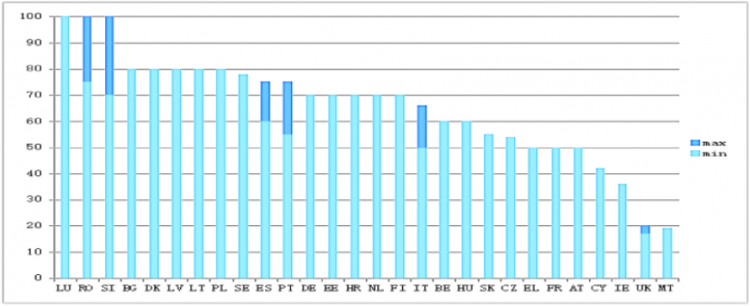
UK SSP is inadequate to meet basic living standards and the low paid have little to no savings to fall back on
Statutory sick pay and social protections for jobless and self-employed people in the UK have breached legal obligations under European law, the Council of Europe has found.
Provisions for the sick and unemployed in the UK were found to be “manifestly inadequate” in a report by the European Committee of Social Rights (ECSR). 15
Statutory sick pay needs to be both adequate and paid over a longer period of time. SSP could function like the Statutory Maternity Pay, the first six weeks 90% of your average weekly earnings then followed by a flat rate over a period of time. This should not be seen as a disincentive in returning to work.
International evidence suggests that changing the incentives and liabilities for employers can be a powerful driver of behaviour16
. Increasing employer contributions to sick pay and lengthening the period of protection can help reduce sickness absence. In the 1980s, employers in the Netherlands only had financial liability for sick pay for a few weeks. This was progressively increased to one year and then two years. This helped incentivise employers to focus on prevention and rehabilitation, thereby reducing sickness absence rates 17
SSP at 28 weeks in the UK can still be insufficient time to recover from some illnesses, though the majority of reasons given for sickness absence in UK are minor illnesses18
. If the length of SSP was increased it would give employees with more serious conditions time to recover rather than fall out of the work place or move on to ESA. The crucial link with employers and the workplace would remain for employees.
It could be with long-term illness over 28 weeks e.g. recovery from cancer or other serious conditions, Government could reimburse employers from that point onwards. This would work in the same way as previously discussed the employer would have to demonstrate good practice in sickness management, and they would have a huge incentive to do so. The Government would have funded ESA or out of work benefits anyway, this approach would just be more effective.
This approach would also avoid those suffering from serious illnesses like cancer not having to apply for Universal Credit halfway through treatment; they do not need any additional stress at this time.
Q27. In your view, would targeted subsidies or vouchers be effective in supporting SMEs and the self-employed to overcome the barriers they face in accessing OH?
Yes – no – maybe – don’t know. Please give reasons for your answer.
Vouchers could be part of an effective solution.
If the public policy problem we are trying to solve is (a) insufficient capacity of specialist and qualified OH services (b) non-engagement by employers in the provision of access to OH services and (c) interventions to sustain the employment of people with chronic health problems, and just as importantly, the identification by OH specialists of workplace practices that are making people ill, and representations to remedy those sources of harm, then we have the following observations:
With reference to (a); vouchers would put money into the demand side for OH services. In parallel there would need to be prior investment in the supply side, workforce planning and training and recruitment of staff. The OH services provided by the NHS to businesses/workers are a quality assured option. It should be noted that when a UK government issued the similar vouchers for adult learning – Individual Learning Accounts – sadly there was widespread abuse and fraud by the private sector, and poor standards and miss-selling, and the facility was quickly withdrawn.
With reference to (b); the cost of OH is already a fully tax-deductible business expense, yet access to OH for workers employed by a business employing fewer than 50 employees is below 10 per cent. There are more reasons than cost for SMEs not providing OH services. Vouchers to employers would raise the rate of engagement of employers but probably not a lot, and from an extremely low base. The government should note that the economies in Europe that are most successful and competitive require employers to provide OH services, including Belgium, Finland, France, Germany and Netherlands. The government should explore the cost and benefits of a simple obligation upon all employers to provide workers with access to multi-disciplinary occupational health services, explicitly including an occupational physician. How this works in other countries should be explored; levies, insurance schemes etc.
With reference to (c); there is a much stronger incentive for a worker to utilise a voucher than an employer. The weakness is this approach however is that there is a risk that structural problems in a workplace regarding job design, intensity of work or hazards, might not be identified and remedies that protect other workers not proposed. So, increasing the effective use of OH services by giving vouchers to workers would need to be aligned with good intelligence gathering and analysis and a in to a re feed-back into a relationship with employers and with workplace health and safety reps.
Q28. Please provide any evidence that targeted subsidies or vouchers could be effective or ineffective in supporting SMEs and the self-employed to overcome the upfront cost of accessing OH services.
Open question.
The prior experience of the abuse of Individual Learning Accounts suggests that there is merit in a system in which vouchers can be ‘cashed’ with NHS OH services, which has accredited standards, quality assured services, and is publicly accountable.
Q29. In your view, would potentially giving the smallest SMEs or self-employed people the largest subsidy per employee be the fairest way of ensuring OH is affordable for all?
- Yes
- No
- Don’t know
- If no or don’t know – what would be better?
We are not persuaded by this. If the focus is on the work and not the business, it is the ‘health difficulty’ that should determine the level of support. Services should be provided to the worker ‘on the basis of need’.
If it is contended that steps to enable a worker with a chronic health problem to sustain their productive employment are generally viable and beneficial to a business; maintaining productivity, minimising absence, avoiding use of agency workers, avoiding new recruitment and training costs etc, then these gains are as tangible for a small employer as they are for a larger one.
Q30. All respondents: what type of support should be prioritised by any potential, targeted OH subsidy for SMEs and/or self-employed people?
- OH assessments and advice;
- Training, instruction or capacity building (e.g. for managers and leads);
- OH recommended treatments.
Yes, all the above. But it is also important that the OH provider feeds-back to the employer such that, where appropriate, employment practices, job design etc, can be amended. The provision of OH services should be a circular, intelligent and learning process. This certainly includes training and capacity building for managers.
However, TUC affiliate unions have told us that there are perverse incentives at work in this arena. For example, the NASUWT told us that NHS OH services regularly fed-back to schools that their employment practices were harmful and should be amended. (This could be about matters such as workload, loss of classroom support services such as teaching assistants or learning support assistants leading to intensification of work, or poor management/bullying and harassment). But the response of some schools was to seek another OH provider, one that did not challenge management practices. We should reflect on whether a private sector OH provider to an employer has a conflict of interest, and whether that contractor will be less likely to report back to the employer robustly about harmful factors at work.
Q31. Please give reasons and details of any other categories of support you think should be included.
As above.
Q32. How could the government ensure that the OH services purchased using a subsidy are of sufficient quality?
The simplest way is for the NHS to be the provider, and then existing quality assurance techniques and accountability systems can be employed and evolved.
If services are offered by the private sector then the offer should include multidisciplinary teams with a breadth of capabilities and clinical leadership, explicitly including a doctor – an occupational physician.
All qualifications should be publicly accredited and moderated.
All OH providers should be proactively inspected and subjected to ‘mystery shopping’ spot tests.
An exemplary and cost-efficient NHS OH service should set the benchmark and be the public sector comparator. NHS OH services must not be allowed to wither.
Q33. As an OH provider, would you be willing to submit information about the make-up of your workforce to a coordinating body? Yes – no – maybe – don’t know.
This should be required, not optional. And it should be complemented by a record of contact time to avoid the phenomenon of ‘consultants’ that have a paper role only; legitimising services provided by lesser, low or unqualified staff.
Q34. If no, maybe or don’t know, what are your reasons for not providing your data?
- time
- cost
- confidentiality
- do not see the benefit
- other – please state
N/A
Q35. As an OH provider, expert or interested party, what are your views on private OH providers’ involvement in the training of the clinical workforce?
- Private providers should be more involved
- Private providers should be more involved but with additional support
- Private providers should not be more involved
The critical points here include; that more OH professionals are recruited and trained, that the training is of a high standard and the qualifications are robust, that the students in training are treated well, they have a defined career and progression paths, they are not tied to an employer and can migrate around the system, that their qualifications are portable, that the correct proportions of OH professionals are trained to staff teams and there are not moves towards a lower quality of OH service provided by less qualified staff.
The qualifications should be public; publicly set, publicly examined, publicly moderated and publicly accountable.
The consultation document acknowledges that effective OH services depend on teams of clinical professionals, the number of which are falling, when need and demand are rising. And the consultation document accepts that private sector OH businesses are, and going forwards will be, reliant on staff that were trained by the public sector, (paragraph 143), that market forces are unlikely to be sufficient to respond to challenges in a timely way, (paragraph 141) and that it will be the public sector that will train new generations of OH professionals.
The OH clinical workforce is declining, there is an acute shortage of OH doctors and OH nurses. 44 per cent of OH providers report staff shortages. But the reality is that it will be the NHS that funds the great majority of new training places.
We agree with paragraphs 144 and 145. There is a need for a strategic oversight, managing and analysing existing data, gathering new data, showing leadership, leading workforce development, coordinating training needs and capacity, and seeking to retain and develop existing OH professionals. And that strategic oversight should be led by the public sector.
The All-Party Parliamentary Group on Occupational Safety and Health, in its report ‘Occupational Medical Workforce Crisis’, 2006, called for:
- The public sector to fund the clinical training posts necessary to meet demand now and in the future.
- New steps taken to ensure staff retention of OH professionals in both the public and private sector.
- Workforce planning for OH must be based on effective teams including OH doctors/occupational physicians; OH services should not be diluted in terms of the balance of skills within teams
- Steps be taken to ensure that all medical schools include OH on the core curriculum, and to promote OH as a career choice.
The consultation document acknowledges the shortage of nurses, that several OH courses for nurses have closed in recent years, and that the number of post graduate OH nurse trainees fell from 200 in 2009 to 80 in 2018, (paragraph 149). Urgent steps should be taken to make a career as an OH nurse more attractive and to make courses more affordable. The bursary for nursing courses should be restored.
Q36. If providers should be more involved but will need support, what additional support would be needed? Open question.
Any private sector organisation delivering OH services, or training OH professionals, new or existing, must meet rigorous standards set and inspected by the public sector. Any poor performance or malpractice by private sector is detrimental to both employers and to workers, but it also damages confidence in the entire sector.
Q37. As an OH provider, expert or interested party, what changes to the training and development of the OH workforce could support the delivery of quality and cost-effective services?
There has been massive under-investment in NHS OH services. Recruitment of doctors into occupational medicine has been falling since 2003, with the number of posts at an all time low. Fewer medical schools include OH in their teaching, very few arrange workplace visits, OH is not portrayed as a dynamic career choice for clinicians, there are fewer and fewer training places. There has been a failure to prioritise, invest in and promote a sustainable OH service within the public sector.
If the OH services provided by the NHS were excellent and ‘in rude health’ structurally in terms of capacity and quality, then private sector OH could work alongside that, if it met the same standards. If the NHS OH service is left to wither and the government expects the private sector to infill for its failure to invest, then the private sector will most likely fail to reach the excellent standards or capacity required. The experience of OH services sector is one of market failure. Excellence in the public sector can lead to effective ‘crowding in’ of third sector and private sector providers, excellence in the public sector will not ‘crowd out’ other providers.
The provision of OH in the UK is an example of market failure. Research shows that investment by businesses in services such as OH, and wellbeing programmes is very effective and value for money in terms of the returns gained; PWC identified a return of £4.17 for every £1 spent by employers on workplace wellbeing programmes. 19
Requiring employers to purchase OH services would build the demand side to balance, and in time fund, the improvements in the supply side offer. We need long-term solutions to the provision of high quality and efficient OH services for all workers who need them.
[19] PWC, Building the Case for Wellness, 2008
Q38. As an OH provider, should there be a single body to coordinate the development of the OH workforce in the commercial market? Yes – no – maybe – don’t know. Please state reasons for your answer.
There must be an inspectorate to ensure standards and quality of experience for learners, it must have enforcement powers. But in terms of workforce planning, there is a need for strategic over-sight and forward planning, and this must include the public sector.
Q39. If yes, what should its role be?
See above.
Q40. As an OH provider, what would encourage providers, particularly smaller providers, to invest in research and innovation in OH service delivery?
Private sector companies are motivated by profit, building market share and building the commercial value of a company, which can be sold. A way to utilise those motivations is to build a bigger ‘market’ for OH services by obliging employers to provide OH services, by some means. It is critical that the NHS is an option for employers as a provider of OH services, both setting standards and acting as a public sector comparator, or provider of first-choice based on trust and efficiency.
Q41. What approaches do you think would be most effective in terms of increasing access to OH services for self-employed people and small employers through the market? Please order in terms of priority:
- New ways of buying OH;
- New OH service models; and
- The use of technology to support OH service provision.
If the purpose of any of the ‘innovations’ referred to above is to deskill the provision of OH services by eliminating OH professionals, especially occupational physicians, it will fail. If the propose is to make high quality OH services available to more workers, then collective solutions, such as insurance or levies upon employers could be part of potential solution.
Q42. If applicable, what other approaches do you think would be effective? Please explain the reasons for your answer.
Government should invest in OH research at universities and institutes, on issues such as the impact of artificial intelligence and working alongside machines in a new status environment on mental health, the OH needs of an ageing workforce, OH and management standards and practices, how to use data to influence employer’s behaviour to build less need for OH services etc. In parallel, government should improve the public sector OH offer to employers and workers. That would be a strong platform for innovation to build upon, using technology, and universities could propose products and services, rather than seeking to use technology as a back-stop to remedy chronic under-investment by employers and the government.
Q43. As an OH provider, expert or interested party, what more could be done to increase the pace of innovation in the market?
- Co- funding;
- Access to finance;
- Help with innovation or evaluation;
- Commercial advice;
- Don’t know;
- Other – please state
If employers were to be obliged to buy OH services, or insurance, or pay a levy, or similar, it would create a demand and a market for products and services.
Q44. As an OH provider, expert, interested party, what methods would you find most helpful for finding out about new evidence and approaches that could improve your service?
More than 90 per cent of workers in Finland and the Netherlands have access to OH services. A good starting point would be to study how this is achieved, and what is the impact of this level of service, and to publicise the findings to all stakeholders.
Q45. As an employer, what indicators of quality and compliance arrangements would help you choose an OH provider?
- Work outcomes;
- Quality marks;
- Process times;
- Customer reviews;
- Other – please state;
- Don’t know;
- Indicators won’t help
Any OH supplier should be required to have current accreditation. Staff to caseload ratios might be informative, similar statistics are used in the university sector. But there is also a dynamic tension here. An employer that is sincere about the fundamental motivations for purchasing OH services, as an ongoing source of intelligence, that informs self-improvement by the employer and change etc, will want to hear honest and challenging feed-back.
- 15https://www.independent.co.uk/news/world/europe/uk-sick-pay-legislation-eu-law-breach-council-europe-social-charter-a8176396.html
- 16https://www.ippr.org/publications/working-well-a-plan-to-reduce-long-term-sickness-absence
- 17https://www.ippr.org/publications/working-well-a-plan-to-reduce-long-term-sickness-absence
- 18https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/employmentandemployeetypes/datasets/sicknessabsenceinthelabourmarket
- 19PWC, Building the Case for Wellness, 2008
Q46. As a provider, what indicators of quality could help improve the standard of services in the OH market?
- Work outcomes;
- Quality marks;
- Process times;
- Customer reviews;
- Other – please state;
- Don’t know;
- Indicators won’t help
See answer to question 45.
Q47. All respondents: how could work outcomes be measured in a robust way?
The key outcome for individual workers is the quality of life.
A key outcome for the state is a cost benefit analysis of the investment in OH services businesses and individuals against the cost of welfare benefits and NHS services, should an individual have to leave employment, and increasing competitiveness/productivity/successful businesses.
The outcome for employers can be measured within sectors by comparing businesses/organisations on a competitor basis, in terms of outcomes such as productivity and health outcomes. Caution is needed with using absence data as a metric; it is not the objective to get workers to go to work when they are ill, which is a form of ‘presenteeism’, nor should we want workers who have chronic health problems to be subject to disciplinaries generated by aggressive absence management packages. Metrics need to be more sophisticated than ‘absence data’.
Q48. All respondents: do you have suggestions for actions not proposed here which could improve capacity, quality and cost effectiveness in the OH market?
Explore a legal requirement for employers to purchase some form of OH cover, or for it to the appended to employer’s national insurance, a levy paid, OH insurance – or similar.
Investment in NHS OH services, especially in the number of training places, recruitment, retention of staff and career progression. In the short-term and medium-term steps need to be taken to seek to incentivise existing OH professionals to stay in the sector, to postpone retirement etc.
Q49. Do you need more information, advice and guidance?
We agree with the point made in paragraph 183; ‘employer behaviour is key’. Employers exhibit a spectrum of attitude to the safety, health and wellbeing of their staff. Some are extremely supportive and progressive and can be exemplars to other businesses, some are weak and need advice, encouragement and support, some avoid their responsibility, actively refusing to engage, some are abusive and exploitative.
Even if the aim of a new strategy is only to raise the provision of OH services and to better maintain the employment opportunities and productivity of some employees, these being the ‘lowest hanging fruit’, there is good cause to do more than provide advice and guidance, but to also provide a degree of ‘challenge’ to employers, to increase the breadth and depth of engagement.
However, if the aim of a strategy is to work to ensure that as near as is possible, all employers engage in this agenda seriously, and all workers have access to OH services if they need them, and all workers have the opportunity to sustain their employment despite having a chronic illness, then the government will need to go beyond voluntarism and introduce changes to the legal framework and elements of compulsion, scrutiny and monitoring of compliance.
Paragraph 184 accepts that employers frequently ‘do not understand their obligations’ in this arena. Consequently, there is virtue in simplicity; such as ‘requiring all employers to provide OH services for their workers’.
Businesses would benefit from best practice models from competitor economies, such as Finland, and Netherlands, and best practice models from UK leaders within various sectors in terms of OH access for workers and successful HR practices. NHS OH services should be vigorously publicised.
Q50. If so, what content is missing?
- Legal obligations and responsibilities/employment law;
- Recruiting disabled people and people with health conditions;
- Workplace adjustments, such as Access to Work;
- Managing sickness absence;
- Managing specific health conditions;
- Promoting healthier workplaces;
- Occupational health and health insurance;
- Best practice and case studies;
- Links to other organisations, campaigns and networks;
- Local providers of services and advice;
- Other – please state.
Employers need to be open to hearing constructive criticism and acting upon it. 1.2 million people who worked in the last year were already suffering from an illness that they believed was caused, or made worse, by their work. 500,000 of these cases were new work-related conditions. The first step towards a world class OH system, and one that is optimally efficient for a company/organisation, is to organise work in such a way that it does not harm people or make them ill. Then our refreshed OH services will only have to address the health needs of workers caused by factors that are exogenous to the workplace.
Q51. What would you recommend as the best source of such new advice and information?
- The main government portal (GOV.UK);
- The Health and Safety Executive;
- Jobcentre Plus; or
- Other – please state.
Advice sources are complementary, but should include HSE, NHS OH services, ACAS, sector bodies and trade unions.
Q52. As an employer, where do you go for buying advice and support when purchasing, or considering purchasing, OH services?
- Internet search;
- Professional/personal contact;
- Legal sources;
- HR person (in-house or external);
- Accountant or other financial specialist;
- Other – please state;
- Don’t know;
- I don’t seek advice or support.
N/A
Q53. As an employer, what additional information would you find useful when purchasing, or considering purchasing, OH services?
- Online questionnaire to help you identify what type of services you could benefit from;
- Toolkit that could include information on OH referral and assessment process;
- Basic online information on the process of buying OH services;
- Provider database;
- Comparison website;
- Information on the value of OH services.
N/A
Q54. All respondents: do you agree with the proposal to introduce a requirement for employers to report sickness absence to government? Yes – no – maybe – don’t know. Please give reasons for your answer.
We agree that good public policy will always be based on good data but quantitative information about sickness absence in isolation from qualitative information about health outcomes and productivity, in an era in which remote working, working from home, flexible working, are increasing – mean that data about sickness absence could be a crude metric. Meanwhile, because of the employment practices of companies that use gig platforms, (companies such as Uber claim to employ very few people), means that any mapping needs to be sensitive to such labour market anomalies.
Q55. As a small or medium sized employer, would you find it helpful to receive prompts to information or advice when you have an employee on a sickness absence? Yes – no – maybe – don’t know. Please give reasons for your response.
N/A
Q56. Do you think this overall package of measures being explored in this consultation provides the right balance between supporting employees who are managing a health condition or disability, or on sickness absence, and setting appropriate expectations and support for employers? Yes – no – maybe – don’t know. Please give reasons for your response.
The general case is that ‘good health is good for business’, and produces better health outcomes for the worker, and a better outcome for the state, avoiding the costs of a person ‘being pushed out’ of the labour market – and potentially on to welfare benefits, greater use of NHS publicly funded services etc. There is a potential ‘win – win – win’ here, a shared interest, rather than a balance of competing interests between a worker and an employer, that it is important to extol if we are to work towards via effective public policy in this arena.
UK residents who are workers deserve access to high quality OH services and the opportunity to sustain their employment. Employers have a legal duty of care to protect the health, safety and welfare of their workers and too few are meeting that duty in full. Many employers who say their ‘most important asset is their people’ do not invest in effective OH services, despite the fact that the evidence suggests that there are tangible commercial gains to be made from effective OH programmes. There is a mutual interest to be secured, and it is one of the foundations of a modern and efficient society and economy, with equal opportunities in the labour market.
Millions of workers in Britain choose to be a member of a union, pay a monthly membership subscription, ask their union to represent them collectively in negotiations with their employer and if need be, to represent them personally. Many of the best schemes that employers/organisations have for OH services have been developed with the active input of unions. Trade union health and safety representatives make an immense contribution to the safety, health and wellbeing of workplaces, as is acknowledged by the government’s own empirical research.
But the important collective role of unions is not recognised in the consultation document. If the OH relationship between an employer and a worker is mediated solely on an individual basis then collective issues will be missed, and sources of collective harm will endure. For example, if process design is leading to musculoskeletal disorders, there is a collective issue. If excessive workload or bad phasing of work is leading to harmful work-related stress, there is a collective issue. If shift patterns are poorly organised, leading to disrupted sleep and all the potential associated long-term health detriments, such as diabetes and heart problems, that is a collective issue. If poor lighting and lack of access to drinking water is contributing to the incidence of migraines, that is a collective issue. Trade union health and safety reps have a key role in identifying hazards, collating individual problems into matters of collective concern, working with employers to eliminate the hazard where possible, and to mitigate where necessary. This role should be recognised and invested in.
Part of the advice and guidance to employers should be about the positive contribution that trade union health and safety reps and collective bargaining make to safety, health and well-being at work, to productivity, and to sustaining the employment of workers who need some form of reasonable adjustment.
Stay Updated
Want to hear about our latest news and blogs?
Sign up now to get it straight to your inbox